Volume 1, No. 1, Art. 28 – January 2000
Involuntary Childless Marriages and the Effects of Reproductive Technology: The Case of Germany
Corinna Onnen-Isemann
Abstract: Since the late 19th century, the proportion of childless couples has increased continuously in almost all industrialized countries. In Germany, this rise was particularly strong. The emergence and continuous development of reproduction technologies triggered a social process, the end of which is not yet foreseeable: In public as well as scientific discussions, the "benefits" of these medical developments have been hotly debated. This wide-ranging coverage of the issue supported the couples' view that they will finally be able to fulfill their wish for a child by means of a reproduction treatment. The article reflects on the social implications of reproductive technologies. On the basis of the author's own study, an integrative model of coping was developed and tested empirically.
Key words: childlessness, stress, coping, reproductive medicine
Table of Contents
1. Introduction
2. The Study
3. Sample
4. Method of Interpretation
5. Several Empirical Findings
6. Coping-Strategies of Involuntarily Childless Married Couples
7. The Process Model of Coping
8. Typology of Coping with Stress
9. Burdens During the Medical Treatment
Since the late 19th century the proportion of childless couples has increased continuously in almost all industrialized countries. In Germany this rise was particularly heavy: In 1989 8.4% of the marriages were childless; by today this rate has risen to 18%. Calculations suggest that as many as 20% of the marriages contracted after 1970 will remain childless for life. The rise in childlessness becomes even more apparent with cohort-specific investigations: While only 9% of the women born in 1935 remained childless, this proportion rose to 20.5% with the 1955 cohort and increased further to 25% with those women born in 1961, with a tendency to rise. It must be emphasized that the proportion of childless marriages would have been even higher if women had not had access to reproduction treatments: the number of those who underwent this kind of treatment has constantly risen over time. [1]
The emergence and continuous development of reproduction technologies triggered a social process, the end of which is not yet foreseeable: In public as well as scientific discussions the "benefits" of these medical developments have been hotly debated. This wide-ranging coverage of the issue supported the couples' view that they will finally be able to fulfill their wish for a child by means of a reproduction treatment. It appears that childless couples consider reproduction technology the only possibility to achieve the goal set by society, i.e. to have a family with children of one's own. [2]
In the German language area theoretical aspects and empirical investigations of medical reproduction technologies have—from a sociological perspective—only been considered in discussions at a relatively late stage. The first texts covering this issue were published in the second half of the 1980s. [3]
But studies focusing real effects of reproductive treatment on the part of involved couples didn't exist in Germany at all. Due to this our study was innovative because we reflected on the basis of the structure of social implications on reproductive technologies. Beyond that we developed an integrative model of coping and tested it empirically. The following article considers the last mentioned topic. [4]
In the following the data collected in an empirical study of the reasons for the increasing demand for medical reproduction technologies in Germany are presented. We followed up this study between May 1993 and December 1995 at the University of Oldenburg, Germany (NAVE-HERZ, ONNEN-ISEMANN & OßWALD 1996). Within this study we collected data of couples who had undergone one or several treatments of medically supported procreation in the course of their lives in a procedure of two levels. First we carried out narrative face-to-face interviews with wives and their husbands. After a content analysis we connected a partly standardized self-administered questionnaire. [5]
Article 6 of the German Constitution in which the state's obligation to support marriage and family is fixed, provides the basis for §27a, section 1, sentence 3 of the social legislation which prescribes that marriage is a prerequisite for artificial insemination (Document of the German Federal Parliament 11/6760, pp.14ff). Therefore our sample contains only married persons. [6]
Because we wanted to acquire the effects of reproductive technologies on marital relations we preferred interviewing one of the partners with its spouse absent. But in some cases the wife wanted to give an interview only in presence of her husband. Only in those cases we accomplished couple-interviews. These interviews show no differences concerning situational aspects so that finally we found out these couple-interviews have been quite successful especially concerning marital authority, the process of decision making and the dyadic coping behavior. [7]
In seven cases we carried out telephone interviews, too. As a result of an advertisement in a women's journal a lot of women replied. Most of them lived far away and therefore we tried telephone interviews which are in Germany mainly used in marketing research. There they replace standardized personal interviews (see BRÜCKNER, HORMUTH & SAGAWE 1982; REUBAND & BLASIUS 1996). We carried out the telephone interviews with the same scheme as we did with the other narrative interviews, always in the early evening and taping the interviews. Their analysis show as well that there was no difference in comparison to face-to-face interviews concerning the frankness. There have been neither problems concerning the confidence of the interviewer nor the topics which are partly very intimate. [8]
In literature we found critique referring to frankness in telephone interviews (see FREY, KUNZ & LÜSCHEN 1990). In contrast to this there was a high anonymous readiness to get interviewed which we explain with an immense strain for women who mostly don't have any possibilities of talking with others about the reproductive treatment—it seems as if we were the only ones with whom they could talk. [9]
After the content analysis of these interviews we developed items as a basis for a partly standardized self-administered questionnaire. Its aim was to prove the stability and the exactness of the results due to the first phase of our research with a broader sample and to gain statistically tested results. [10]
The sample of the first phase of our study contains 52 narrative interviews with women and men who had undergone one or several treatments of medically supported procreation in the course of their lives. 30 of these interviews have been face-to-face interviews with women, 15 of them have been couple-interviews; to be added with 7 telephone interviews with women. All interviews were carried out between November 1992 and June 1995. [11]
We assumed that all women who undergo a reproductive treatment are unvoluntarily childless at the beginning of the treatment. Contrary to this assumption we found two groups of women under treatment:
the "primary-childless women" had never born a child, and
the "secondary-childless women" who had already born a child and who can't realize another wish for a child.1) [12]
According to this definition our narrative sample contents eight "secondary-childless" women and 44 "primary-childless" women, eleven of them had already born a child due to reproductive treatment. [13]
The survey by self-administered questionnaires took place between May 1994 until December 1995, we collected 273 questionnaires. Nearly half of the respondents have been under reproductive treatment (n=130), almost ¼ either dropped the treatment without success or ended it for other reasons (n=66). ¼ carried out successfully the reproductive treatment, for example a respondent was pregnant or did already give birth to a baby (n=51), the other respondents found themselves at the very beginning of the treatment. All educational levels were represented, the higher ones lightly dominated. [14]
In this study we used the method of triangulation of a plurality of research. The first step included the content analysis of the qualitative interviews. Due to the lack of methodological and systematical criteria concerning methods of interpreting transcribed interviews we used several "proven" procedures and combined them. Therefore I chose first as method of interpretation of narrative interviews a phenomenological position: the material analysis of interpretation patterns (KADE 1983, pp.112ff.), and supplemented "six steps of interpreting autobiographical off-hand-stories" according to SCHÜTZE (1983, pp.286f.). These are
the formal text analysis, in which non-narrative elements are removed,
the structural description of partial contents,
its abstract analysis,
the analysis of knowledge with the aim of elaborating a dominant processual structure,
contrastive comparisons of several similar cases in order to evaluate theoretical structures of alternative options of action, and finally
the construction of a theoretical model to combine the steps of interpretation systematically and analytically (cf. SCHÜTZE 1983, pp.286f., SANDER 1997, pp.70ff.) [15]
The results due to these described methods have been proven in a further step with the data of the second phase with frequency analysis of configuration patterns, which I finally reflected again with the qualitative material by means of case studies (MAYRING 1988, 1993, p.27). [16]
I mainly used the data collected by questionnaires for interpreting the theoretical model of coping with infertility. We studied theoretical differences of relevant parts of strain during the phase from diagnosis to the beginning of a treatment program before carrying out narrative interviews. Within the interview situation we directed the focus on the individually experienced stress events and confronted the respondents with a progress scheme, which contained theoretical findings concerning the progress of strain in terms of statements. The respondents were asked to comment on each point. This procedure allows two kinds of getting data: first the respondents were able to talk about their individually experienced burdens—no matter if before getting the medical diagnosis or afterwards—and second they could argue directly by the scheme of process with their burdens after getting the diagnosis. So the scheme of progress has had two functions. [17]
An early finding of the study was that the reasons for getting married given by those who were unable to realize their wish for a child did not differ from those reasons indicated by couples who had children after getting married: The reason which all of the interviewees gave was to have children, which means that at marriage most of the couples did not yet know that they could not have children. Initially the realization of their wish for a child was postponed. Owing to gynecological or andrological changes that occurred (illness due to age or psychosomatic illnesses) voluntary temporary childlessness may lead to involuntary childlessness. This was the case with 62% of the women interviewed who eventually started a reproduction treatment. Hence medicine has brought about a paradox: after effective contraceptives to avoid pregnancy have been developed, today many women can only overcome the inability to procreate and involuntary childlessness respectively with the help of modern medical technologies. Those seeking to overcome childlessness were under pressure because it was their wish to set up a "standard family" with a child of their own. When they finally decided to have a child they had reached an age at which the ability to have a child is reduced. [18]
The fact that so many women postponed a pregnancy allows the assumption that they did so only because they knew about modern reproductive technologies. Their reasons for postponing vary broadly, as the following table shows:
|
Reasons |
In % |
|
Concerning profession |
60,5 |
|
Partner didn't want children |
36,1 |
|
We didn't want to take responsibility for a child |
27,4 |
|
Children restrict one's personal freedom |
24,6 |
|
In education/ training, no financial security |
8,6 |
|
Partnership was too young |
4,9 |
|
We had to build up an economical base |
3,7 |
|
Too young for children |
3,7 |
|
Fear, that matrimonial relationship could suffer |
2,9 |
|
multiple response of N |
162 |
Fig. 1: Reasons for contraception at the beginning of the marriage [19]
The interviews with patients of reproductive medicine show that many of them had internalized a concept of a mother and family role which is inconsistent with their professional orientation but seems to have still a major meaning for their life planning: all the interviewees talked without being asked about a mothers employment and the respective combination of job and family (cf. NAVE-HERZ 1988). When we asked about their future life goals at the youth age all of them said that they had wanted to have a child at some time. At those times as well as today they obviously orient towards the female "normal biography": marriage is considered as presupposition for the later birth of children, who again by some cause a complete or at least partial employment interruption (cf. LEVY 1977, p.44). [20]
It can be assumed that the new offer "reproductive medical treatment" causes a different behavior concerning adoption in Germany: if an own child belongs to the normality of a marriage and a birth is impossible, then people try other ways to reach their goal and to correspond with the normality patterns. Only about 20 years ago people had to come to terms with not becoming pregnant—the only chance for a child and to correspond with family concepts was the adoption (HOFFMANN-RIEM 1989, p.35). The ongoing development of reproductive technologies nowadays could promote a "pre-transfer" of control of family building processes in order to reach a kind of normality within the phase of procreation. So—as for the respondents—the normality could be reached very soon. [21]
The great number of women who undergo reproduction treatments reflects the importance that is still attributed to the "nuclear family" (parents with children of their own) and the high priority that is given to the role of a mother, despite the great variety of lifestyles in today's society. 35% of the female patients indicated that it was their wish to have children and that they took the initiative when the decision of whether or not to undergo a reproduction treatment was made (cf. VAN BALEN & TRIMBOS-KEMPER 1995, pp.140f.). Only in 3% of the cases the husband forces his wife to undergo a treatment. 53% stressed out the conformity within the partnership of their wish for a child. However it can't be spoken of the couple as a motor for reproductive medicine because only a few husbands took the active part and convinced their wife to undergo a treatment, as more than 34% of the wives did! [22]
Above all older women didn't want to wait anymore and started the treatment on their own. There were more younger couples and those with lower educational level who stressed their common decision (cf. RAUCHFUSS 1998, p.229). [23]
6. Coping-Strategies of Involuntarily Childless Married Couples
These data support the results obtained in other studies. Undergoing a reproduction treatment causes a lot of stress and is a major event in a woman's life (cf. VAN BALEN, NAAKTGEBOREN & TRIMBOS-KEMPER 1996; summary of ONNEN-ISEMANN 1995). Each step of the treatment raises new uncertainties among the couple, especially because the doctors cannot predict whether the treatment will be successful. [24]
The burdens to which those undergoing a medical treatment are exposed may be found at different stages: whilst on the individual stage the patient has to compensate directly the physical effects of the medical treatment as well as to maintain a great temporal and organizational expenditure concerning the treatment the marital relationship may suffer. Both know the background that in Germany a maximum of 20% of the treatments of the year 1996 were successful (FELBERBAUM & DAHNKE 1997, pp.102ff.)! On the stage of other social relationships, the couple has to cope with reactions from family members, friends and acquaintances. [25]
Beyond that the burdens may be divided into objective and subjective ones. The objective burdens are a major expenditure of time and organization: the couples have to perform the progenetive act at a fixed date; moreover the couples have to tune the dates for gynecological examinations and for the taking of blood samples with the medical practice and their own working time. In many cases working women use all the holidays of one year for the treatment in order not to lose their job. [26]
The subjective strain to which those undergoing a reproduction treatment are exposed are much more unpleasant: the emotional relationship between the partners and towards the social environment is affected; too much importance is given to the individual steps of the treatment and—in some cases—personal interests are given up entirely. These are only some of the possible consequences of a reproduction treatment (see SCHUHRKE 1993, pp.252ff.). [27]
In addition to these burdens, structurally caused strain in terms of medical intervention has to be noticed. Each partial step of the treatment is combined with a new uncertainty on the part of the couple but also on the part of the gynecologists due to the unpredictability. Above all the couples feel subjective psychological strain combined with helplessness. [28]
Concerning this emotional stress the question of coping-strategies arises. The diagnosis of sterility or infertility means for most of the couples a growth of psychological strain that has to be coped with. I assumed that at different times during the process of wish for a child respondents react in different ways to this. [29]
The decision to undergo a reproduction treatment has many implications and frequently is the beginning of a long period of emotional strain for the men and women affected. The major question to be tackled is how men and women cope with the burdens accompanying the reproduction treatment. Two phases—characterized by different extents of strain—must be differentiated: the period before entering a reproduction program, i.e. the time during which the couples realize that a pregnancy cannot be brought about, up to the beginning of the treatment, and the time during which the persons affected undergo a reproduction treatment up to its completion. [30]
A great number of the women interviewed, who had undergone a reproduction treatment, had been trying to get pregnant for a long time. Before making the decision to start a reproduction treatment these women had already gone through several unpleasant "stages": at first the hope of getting pregnant, then the realization that either the man is sterile or the women cannot have children and finally the psychological reaction that is triggered. Two reactions are conceivable: Either childlessness is not accepted as fate or it is considered a reason to find a new orientation in life. [31]
During this process the result of this perception is interesting due to its intensity and in its consequences on the following treatment, the perception of stress events in future and probably on the partner and his or her way of dealing with the wish for a child. After a couple has been diagnosed infertile, and sterile respectively, by a gynecologist or andrologist, the psychological and social responses to this diagnosis widely differ, depending on an individual's competence for action. From the perspective of action theory a person's behavior is determined by his or her perception of and reaction to the environment and vice versa. These individual reactions become part of a person's action resources (cf. HURRELMANN 1988, pp.95ff, GUTTORMSEN 1992, pp.249ff., see HÖLZLE 1988, CALLAN & HENNESSEY 1989) and determine his or her competence for action. [32]
7. The Process Model of Coping
According to this linear model of coping with involuntary childlessness, the first phase—after having been faced with the diagnosis of infertility/insterility is a shock. The couple realizes that having children of their own is not an option any more, that they have to make plans for a life without children. In many cases the reaction to this new prospect is despair and hopelessness. [33]
The second phase is dominated by a feeling of non-acceptance: the couple refuses to accept the diagnoses. The individual's self-esteem and self-image are called into question and the couples affected undergo one or several reproduction treatments in order to revise the diagnosis. This seems to be a state of "exhaustion, which prevents any emotional freedom and restricts love of live" (GUTTORMSEN 1992, pp.250). [34]
The next phase is dominated by anger and rage. Frustration that occurs after many visits to the doctor and unsuccessful reproduction treatments alternates with aggressions e.g. against couples with children. One's own insufficiency may cause irrational reactions to one's entire social environment. In the course of the fourth phase which is dominated by feelings of guilt and shame many couples search their past in order to identify the causes of their insufficiency. Many couples consider the former use of contraceptives or abortions they have had, or escape into religious beliefs a possible explanation for their infertility and sterility respectively. Sometimes the reactions are—subconsciously—directed against one's partner, e.g. the partner who is fertile/procreative shows grief over the situation and in this way makes his/her partner who is infertile/sterile feel guilty. [35]
During the phase of isolation (5) the couples almost withdraw completely from all those social contacts which are—directly or indirectly—associated with children. After this they go through a phase (6) that is dominated by depressions . Mostly women seem to suffer from depressions because they often believe that they are to blame for childlessness; they lose interest in everyday-life, suffer from sleeplessness and are hardly interested in their work (cf. GUTTORMSEN 1992, p.251). [36]
Hereafter the phase of grief (7) begins. The paralyzing depressions are replaced with feelings of sorrow which trigger a process of coping with the situation, e.g. couples start to make new plans for the future and get used to the idea that they will never have children of their own. In the final phase the diagnosis "infertility and sterility", respectively is finally accepted and the lethargy disappears. Only then, after the persons affected have gone through all these phases will the couples be able to make major decisions for their future lives, e.g. they decide to undergo a medical reproduction treatment (cf. also HURRELMANN 1988, pp.96ff., BODENMANN & PERREZ 1993, pp.181ff, STRAUß et al. 1991, p.97 on the course of the phase model, ONNEN-ISEMANN 1996, 1999). [37]
This progress provides the complete coping of each phase of a stressful event before the individual is able to start with real steps to influence its effects. In other words: all steps of coping should be finished before starting a medical reproductive treatment. So it is likely that the respondents are obvious of the different options they have, of what only one is the beginning of a reproductive treatment. But our study revealed that involuntarily childless couples do not go through all phases of the model in order to be ready to take concrete measures for overcoming childlessness—one of which is to undergo a reproduction treatment: In our empirical study many women skipped a phase and tried to cope with the situation in different ways before they started a medical treatment. Van BALEN and TRIMBOS-KEMPER found similar results in their studies. They stress: "Infertility seems indeed a life-long experience. It looks like time does not heel the wounds, in this case. In every life stage there will be confrontations with infertility (getting children, watching children growing up, seeing children leave home, getting grandchildren) and the social world of people who have children" (VAN BALEN & TRIMBOS-KEMPER 1994, p.162). [38]
It was striking that many of the couples surveyed skipped the final phase of acceptance of childlessness and started to undergo a reproduction treatment immediately. As a result coping with childlessness was a process which the couples lived through parallel to the medical treatment. This is particularly dangerous because the persons affected focus all their hopes on getting a child by means of the reproduction treatment and in this way they put off the digestion of their own insufficiency so that ultimately life without children appears to be inconceivable. The couples are convinced that there are no other solutions to their problem.
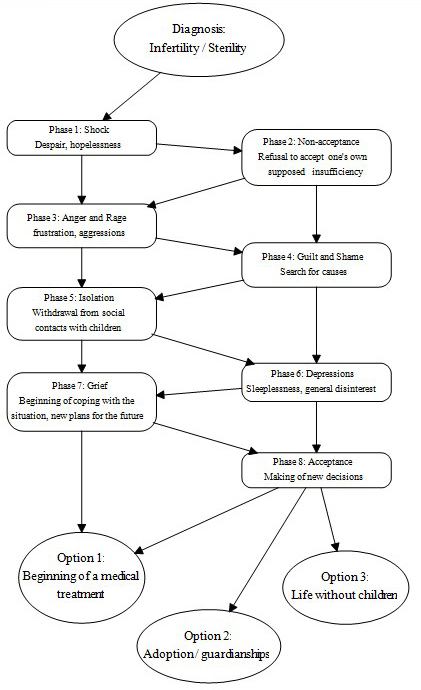
Fig. 2: Model of coping with stress [39]
8. Typology of Coping with Stress
These steps might not be consecutive or urgently necessary. However—as our study reveals—they are not changeable, neither in the quantitative nor in the qualitative parts of the research. Similar frequencies show that the interviewees respond in terms of patterns and vary in their coping strategies. Concerning the comprehensive process of coping with eight steps—as shown above—I assumed as many different coping patterns as there were respondents in the sample. But instead, though I had a relatively small sample in comparison to a statistical analysis, there were only 67 different configuration patterns, on an average four persons have the same coping strategy! [40]
The question that occurs is whether there a typical course of coping steps. Different statistical analysis methods, such as frequency analysis of configuration patterns, of interaction structures and predictive configuration analysis were applied. These statistical operations confirmed the existence of respondent-patterns and resulted in two statistical types of coping:
Type 1 includes the configuration pattern "Shock", "Non-acceptance", "Anger and Rage", "Isolation", "Depression" and
Type 2 the configuration pattern "Shock", "Anger and Rage", "Isolation", "Depression", "Acceptance". [41]
Finally the method of triangulation could ensure these types of coping empirically. [42]
9. Burdens During the Medical Treatment
Considering the various burdens described above to which the couples are exposed, the question arises of how the patients cope with the stress of the treatment and why men and women complete the treatment despite the strain involved. Is it possible that there is a third party involved which influences the couple's decision to undergo a reproduction treatment? [43]
When asked about the support they get, most of the women answered that their husbands helped them to pursue this "solution". Although 16% of the men described their attitude towards the treatment as "reserved" or "tolerating", 96% of the women indicated that their husband was the person with whom they talked most about the treatment they undergo; gynecologists ranked second (65%). 92% of the women pointed out that their husbands had responded positively to the treatment. Of these women 80% described their husbands reaction as extremely positive and 14% stated that their husbands had reacted very positively. [44]
As mentioned above, the couples interviewed also received support from gynecologists who encouraged them to complete the treatment despite the strain involved. 84% of the women stated that the encouragement by doctors was a great help to them. 60% said that they would not have started another treatment if they had not been encouraged by the attending physician. Only a small number of interviewees pointed out that they had been encouraged to undergo a reproduction treatment by "external sources", e.g. by media reports. [45]
It might be assumed that the decision in favor of or against a reproduction treatment was closely linked to the person's family of origin, particularly because childless men and women had been exposed to discrimination from this side. However, our studies revealed that the families of the persons affected hardly play a role in the decision making process; if family members are mentioned at all, these are female. More frequently, the men and women considering a reproduction treatment ask friends and acquaintances for advice. [46]
From a sociological perspective this behavior seems to be comprehensible because sexuality-related issues and problems in Germany are very frequently tabooed or suppressed within families. "The reproduction treatment is considered an intrusion into one's most intimate sphere so that most of the couples are anxious to hide it from their environment" (BRÄHLER 1995, p.182; translated by C.OI). In summary it can be stated that approx. 32% of the women surveyed in our study only discussed the treatment with their husband and gynecologist, respectively, but with no other person. Considering that the women surveyed were a random sample who had volunteered to be interviewed and were therefore willing to talk about their reproduction treatment, it can be assumed that actually the proportion of those who conceal this treatment is much bigger than the rate which our interviews yielded. [47]
In view of the great psychological and physical strain involved in a reproduction treatment the question that poses itself is why the couples undergo a second, third or even fourth treatment if the first treatment has not been successful. [48]
A major reason given by the women surveyed for continuing the treatment was that they were afraid of suffering from self-reproaches later on if they did not make several attempts to overcome childlessness. In the questionnaire which the sample completed, 79% (n=187) of the women affirmed the following statement: "Although I did not feel well during the different phases of the treatment I will not drop out because I do not want to have to blame myself afterwards for not having made several attempts." From this perspective the treatment may take on an "addictive nature" for the patients (BRÄHLER 1995, p.183). BECK-GERNSHEIM wrote: "... Those who give up before having undergone the most recent treatment (a circle without end) have to "blame themselves". They could have made another effort. In this way reproduction technology becomes a reproduction ideology." (1991, p.55; translated by C.OI). The couples make a "benefit-cost analysis", i.e. the decision making process of whether to drop out of a treatment if one does not get pregnant or to continue the treatment is dominated by the fear that one might regret the decision (to drop out) afterwards and by exaggerated hopes for a successful outcome of the treatment. The "benefit", i.e. to get pregnant eventually, seems to become the more desirable the more the individuals have "invested", i.e. the more the couples have exposed themselves to organizational and physical strain. It can be assumed that this is the reason why 77% of the sample affirmed the following statement: "From every single step (of the treatment) I derive new hope for the next". These hopes of the women makes one think of a lottery. Just like in a lottery, where the chances of winning are very limited, the success rate of reproduction treatments is low: per year only 20% of couples undergoing such a treatment may "take a baby home" (FELBERBAUM & DAHNKE 1997, pp.102ff.)! This low success rate does not prevent couples from trying to start a family. Options which childless couples had in the past, such as to adopt children (born out-of-wedlock) or to take on children from poor families with many children (in general these children were given to rich childless relatives), are not available any more. The possibilities of adopting a child have been reduced significantly; frequently—just like foster children—adopted children are not considered an adequate substitute for a child of one's own. Only 25% of the women surveyed seriously considered adopting a child. They would do so only if several reproduction treatments had turned out unsuccessful! Thus it becomes clear why the reproduction technology is in general considered the only possibility of achieving the cultural goal of "starting a family, entering parenthood", at least as long as this goal itself is not called into question. [49]
1) In contrast to this definition physicians differ between "primary sterility", "infertility", and "secondary sterility". "Primary sterility" means that the woman can't get fertilized (independent of the reason, i.e. the wife or the husband), "infertility" describes the impossibility to deliver, and "secondary sterility" the impossibility of another ferlilization after an earlier conception (STAUBER 1993, p.55). The main users of reproductive treatment belong with 60.6% to the first group of "primary sterility". Due to the authors definition of "primary-childless women" this group contents women, who are either sterile or infertile respectively whose husbands are sterile; the group of "secondary-childless women" contents women, too, who had already born one child or even more. <back>
Beck-Gernsheim, Elisabeth (1991). Technik, Markt und Moral—Über die Reproduktionsmedizin und Gentechnologie. Frankfurt/Main: Fischer Taschenbuch Verlag.
Bodenmann, Guy & Perrez, Meinrad (1993). Streß- und Copingdiagnostik in Partnerschaft und Familie. Zeitschrift für Familienforschung, 5(3), 177-214.
Brähler, Christa (1995). Fertilitätsstörung—Kränkung und Herausforderung. In Elmar Brähler (Ed.), Körpererleben: ein subjektiver Ausdruck von Körper und Seele. Beiträge zur psychosomatischen Medizin (pp.181-186) (2nd ed.). Gießen: Psychosozial-Verlag.
Brückner, Erika; Hormuth, Stefan & Sagawe, Helmuth (1982). Telefoninterviews—Ein alternatives Erhebungsverfahren? Ergebnisse einer Pilotstudie. ZUMA Nachrichten, 11, 9-36.
Callan, Victor J. & Hennessey, John F. (1989). Strategies for coping with infertility. The British Journal of Medical Psychology, 62(4), 343- 354.
Felberbaum, Ricardo & Dahnke, W. (1997). Deutsches IVF-Register. Ergebnisse der Datenerhebung für das Jahr 1996. Fertilität, 13, 99-112.
Frey, James H.; Kunz, Gerhard & Lüschen, Günther (1990). Telefonumfragen in der Sozialforschung. Opladen: Westdeutscher Verlag.
Guttormsen, Gro (1992). Unfreiwillige Kinderlosigkeit: ein Familienproblem. Praxis der Kinderpsychologie und Kinderpsychiatrie, 41(7), 247-252.
Hoffmann-Riem, Christa (1989). Das adoptierte Kind: Familienleben mit doppelter Elternschaft. (3rd ed.). München: Fink.
Hölzle, Christine (1988). Probleme des unerfüllten Kinderwunsches und seiner medizinischen Behandlung. In Gertrude Pauritsch, Beate Frankele & Elisabeth List (Eds.), Kinder machen. Strategien der Kontrolle weiblicher Fruchtbarkeit (Vol.6, pp.10-21). Wien: Wiener Frauenverlag.
Hurrelmann, Klaus (1988). Sozialisation und Gesundheit. Somatische, psychische und soziale Risikofaktoren im Lebenslauf. Weinheim, München: Juventa.
Kade, Sylvia (1983). Methoden des Fremdverstehens. Ein Zugang zu Theorie und Praxis des Fremdverstehens. Bad Heilbronn: Klinkhardt.
Levy, Rene (1977). Der Lebenslauf als Statusbiographie. Stuttgart: Enke.
Mayring, Philipp (1988). Qualitative Auswertung im Rahmen des Belastungs-Bewältigungs-Paradigmas. In Brüderl, Leokadia (Ed.), Theorien und Methoden der Bewältigungsforschung (pp.200-207). Weinheim, München: Juventa.
Mayring, Philipp (1993). Einführung in die qualitative Sozialforschung. (2nd ed.). Weinheim: Beltz Verlag.
Nave-Herz, Rosemarie (1988). Kinderlose Ehen—eine empirische Studie über die Lebenssituation kinderloser Ehepaare und die Gründe für ihre Kinderlosigkeit. Weinheim, München: Juventa.
Nave-Herz, Rosemarie; Onnen-Isemann, Corinna & Oßwald, Ursula (1996). Die hochtechnisierte Reproduktionsmedizin—Strukturelle Ursachen ihrer Verbreitung und Anwendungsinteressen der beteiligten Akteure. Bielefeld: Kleine.
Onnen-Isemann, Corinna (1995). Ungewollte Kinderlosigkeit und moderne Reproduktionsmedizin. In Bernhard Nauck & Corinna Onnen-Isemann (Eds.), Familie im Brennpunkt von Wissenschaft und Forschung (pp.473-488). Neuwied: Luchterhand.
Onnen-Isemann, Corinna (1996a). Handlungsorientierungen ungewollt kinderloser Frauen und reproduktionsmedizinische Behandlung. In Hans Peter Buba & Norbert F. Schneider (Eds.), Familie—Zwischen gesellschaftlicher Prägung und individuellem Design (pp.261-272). Opladen: Westdeutscher Verlag.
Onnen-Isemann, Corinna (1996b). Ungewollte Kinderlosigkeit und ihre Auswirkungen auf die Ehebeziehung. In Friedrich W. Busch & Rosemarie Nave-Herz (Eds.), Ehe und Familie in Krisensituationen (pp.117-136). Oldenburg: Holzberg.
Onnen-Isemann, Corinna (1999). Wenn der Familienbildungsprozeß stockt... Eine empirische Studie über Streß und Coping-Strategien reproduktionsmedizinisch behandelter Partner. Habilitationsschrift, Universität Magdeburg.
Rauchfuß, Martina (1998). Die Kinderwunschpatientin? Das Kinderwunschpaar! psychomed, 10(4) 229-235.
Reuband, Karl-Heinz & Blasius, Jörg (1996). Face-to-face, telefonische und postalische Befragung. Ausschöpfungsquoten und Antwortmuster in einer Großstadtstudie. Kölner Zeitschrift für Soziologie und Sozialpsychologie, 48(2), 296-318.
Sander, Dirk (1997). Warum (noch) ledig? Warum nicht Ehe? Bielefeld: Kleine.
Schuhrke, Bettina (1993). Psychische Probleme bei der medizinischen Unfruchtbarkeitsbehandlung und ihre Bewältigung: Ein Überblick. Verhaltensmodifikation und Verhaltensmedizin, 14(3), 244-270.
Schütze, Fritz (1983). Biographieforschung und narratives Interview. Neue Praxis, 283-295.
Stauber, Manfred (1993). Psychosomatik der ungewollten Kinderlosigkeit. (3rd ed.). Berlin: Berliner Medizinische Verlagsanstalt.
Strauß, Bernhard; Argiriou, Christos; Buck, Sybille & Mettler, Lieselotte (1991). Die In-vitro-Fertilisation im Rückblick: Subjektives Erleben und psychische Folgen im Urteil betroffener Paare. In Elmar Brähler & Annelore Meyer (Eds.), Jahrbuch der medizinischen Psychologie (Vol.5, pp.89-109). Berlin, Heidelberg: Springer Verlag.
Van Balen, Frank & Trimbos-Kemper, Trudy C. M. (1993). Long-term infertile couples: a study of their well-being. Journal of Psychosom. Obstet. Gynecol., 14, 53-60.
Van Balen, Frank & Trimbos-Kemper, Trudy C. M. (1995). Involuntary childless couples. their desire to have children and their motives. Journal of Psychosom. Obstet. Gynecol., 16, 137-144.
Van Balen, Frank; Naaktgeboren, Nico & Trimbos-Kemper, Trudy C. M. (1996). In-vito fertilization: the experience of treatment, pregnancy and delivery. Human Reproduction, 11(1), 95-98.
Corinna ONNEN-ISEMANN
Contact:
Priv. Doz. Dr. habil. Corinna Onnen-Isemann
Heideweg 44
26160 Bad Zwischenahn, Germany
Phone: +49 / (0)441 – 691 407
Fax: +49 / (0)441 – 699 0117
E-mail: C.Onnen@uni-oldenburg.de
Onnen-Isemann, Corinna (2000). Involuntary Childless Marriages and the Effects of Reproductive Technology: The Case of Germany [49 paragraphs]. Forum Qualitative Sozialforschung / Forum: Qualitative Social Research, 1(1), Art. 28, http://nbn-resolving.de/urn:nbn:de:0114-fqs0001289.
Revised 3/2007

Creative Commons Attribution 4.0 International License