Volume 10, No. 2, Art. 17 – May 2009
Assessing the Quality of Qualitative Health Research: Criteria, Process and Writing
Carlos Calderón Gómez
Abstract: The debate surrounding the assessment of quality in qualitative research becomes particularly relevant in the field of Qualitative Health Research (QHR). The characteristics of both its theoretical implications and the practical use of its results support the need for defining shared coordinates for quality assessment that respond to both the methodological requirements and the substantive components of QHR. From this I considered identifying three dimensions: criteria, process and writing. These have frequently been intermingled in previously published QHR quality assessment proposals. Aiming at integrating the development of new and necessary contributions, my explanation of these dimensions and the relationships among them is based on a wide-ranging review of published literature.
Key words: qualitative health research; quality assessment; quality criteria; critical appraisal
Table of Contents
1. Introduction
2. From the Difficulty of Total Consensus to the Need for Partial Consensuses
3. Criteria, Process and Writing
3.1 Criteria
3.2 Process
3.3 Writing
4. Relationship Between Dynamics and Levels in QHR Quality Assessment
5. Conclusions
Quality assessment is widely considered to be highly relevant in Qualitative Health Research (QHR), and has therefore become the focus of numerous debates and publications. The following contribution is based on my teaching, research, and clinical experience in the field of primary health-care, as well as on a wide-ranging literature review on the topic. I do believe in the possibility of improving research practice through meaningful discussion. With a focus on this goal, in this paper I will discuss three main axes of analysis. The first axis concerns the characteristics of QHR as a field where areas of consensus regarding quality assessment must be sought. The second axis deals with the advisability of distinguishing three dimensions frequently intermingled in previously published QHR assessment proposals: criteria, process, and writing. Finally, I will support the relevance of considering not just those three dimensions individually, but also the dynamics of their interconnections in the assessment task. [1]
2. From the Difficulty of Total Consensus to the Need for Partial Consensuses
Plurality is one of the main traits of both qualitative research (QR) in general and QHR in particular. Despite providing undeniable opportunities for openness and mutual enrichment, this plurality of trends and approaches, methods and disciplines, languages and interests can also lead to numerous difficulties for mutual understanding and even some degree of frustration when realizing that the distance among interlocutors might sometimes be greater than the extension of the areas held in common. [2]
At the theoretical-epistemological level, the scope of approaches runs from the most relativistic and post-modern to the most realist perspectives, including multiple versions of critical thinking. The numerous attempts to classify these approaches are, by themselves, proof of this diversity. In some cases, these attempts are situated at the level of knowledge "paradigms"; for example, positivism, post-positivism, critical theory, constructivism, participatory practice paradigm, interpretive paradigm, and pragmatism (GUBA & LINCOLN, 2005; VASILACHIS DE GIALDINO, 2006; CRESWELL, 2007). In other cases, classifications are located at the level of "perspectives," "trends," "methodological approaches" or "methods" (VALLÉS, 1997; MERCADO, LIZARDI & VILLASEÑOR, 2002), thus showing a very wide and diverse range of options depending on different authors' points of view: case studies, ethnography, phenomenology, ethnomethodology, grounded theory, biographical method, historical method, action research, clinical research, ethnoscience, discourse analysis, evaluative research, and narrative research (DENZIN & LINCOLN, 1994; MORSE, 1994; RODRÍGUEZ, GIL & GARCÍA, 1996; ÍÑIGUEZ, 1999; CRESWELL, 2007). This diversity is also present in the most recent attempts at synthesis, which endeavor to link research traditions and qualitative approaches with their disciplinary origins (SPENCER, RITCHIE, LEWIS, DILLON & NATIONAL CENTRE FOR SOCIAL RESEARCH, 2003). [3]
The characteristics of those disciplines that have incorporated qualitative approaches to their theory and research production processes (e.g. sociology, psychology, linguistics, anthropology, medicine, and nursing) constitute an important plurality-increasing factor. Researchers are now more often able to find examples of the benefits of interdisciplinary collaborations which help to reduce the commonly encountered excessive subdivisions of knowledge. However, it is also far too easy to find experiences related to a lack of communication resulting from a greater or lesser degree of entrenchment in the academic or practical worlds, and the use of specialized disciplinary discourses, as well as conflicts of interest and power struggles (CHAPPLE & ROGERS, 1998). These power struggles also vary according to the degree of fluency in dominant languages, notably English, and bring along asymmetries in efforts, costs, and flows of information, pointing out generally English-speaking regions. [4]
The development of QR in the past few decades has brought about the emergence of new approaches and trends, all of which are difficult to categorize into a single model (DENZIN & LINCOLN, 2005), as well as numerous exchanges of influences and experiences that have given more plasticity and flexibility to QR practice. Consequently, in addition to research studies explicitly located in one of those numerous theoretical trends, we also come across experiences reflecting the "cognitive pluralism" supported by authors such as BELTRÁN (1986). In these cases, contributions from more than one tradition or trend are collected without undermining the theoretical and methodological coherence that should characterize research work. ATKINSON (1995) has been long warning us about the risks associated with holding rigid and closed views on trends and paradigms. It is still quite common to view these as a series of one-way streets, only one of which the researcher is permitted to follow. In my opinion, references to different theoretical, philosophical, and sociological trends should not be rigidly understood, nor should they be reduced to some form of "formal labeling" far from that which is researched and the researcher's reality. To the contrary, they should work as sources of training and information, necessary and plural at the same time, for the adequate support of the methodological options to be adopted for specific goals and in specific contexts. [5]
Focusing on quality assessment, the already mentioned diversity of trends and traditions makes it very difficult, and likely not viable, to hope for a common set of approaches regarding the quality of QR as a whole. In fact, different authors have now chosen to transfer those different theoretical perspectives onto the field of quality assessment (SMITH & DEEMER, 2000; PATTON, 2002; CRESWELL, 2007). [6]
However, it is likely as the domains of QR become more narrowly defined that the aims of research projects and the values and views of the audience gain further relevance as key issues in the process of setting guidelines for QR assessment. In the case of QHR, these aims and audiences are, to a great extent, quite unique, especially when entering the field of health care provision. That is, without forgetting that neither health nor QHR as objects of study can be set apart from the previously outlined theoretical and epistemological considerations (DE SOUZA MINAYO, 1995; RATCLIFFE & GONZÁLEZ DEL VALLE, 2000), we also need to acknowledge the influence of its extraordinary growth in underlining some characteristics specific to QHR. In my opinion, these features help to reduce the distances between interlocutors in their search for common spaces and reaching consensus in the field of quality assessment. [7]
As MORSE (2007a) has argued, this level of research production has illustrated the importance of the contribution of QHR to the understanding of the meanings of health and illness for different populations, caregivers, and service providers, as well as their links to family, community, and institutional contexts, both urban and rural. Its development has also reached areas, such as public health (ULIN, ROBINSON & TOLLEY, 2005) and health technology evaluation (MURPHY, DINGWALL, GREATBATCH, PARKER & WATSON, 1998; LEYS, 2003), that were, until recently, exclusive to epidemiology and statistics. This growth has also clearly shown the need to adapt QR methods and techniques to the specific characteristics of those research aims and contexts (MORSE, 2007b). [8]
It should also be kept in mind that although the "qualitative gaze" has always been implicit in good clinical and health-care practice (CONDE, 2002) its methodological development was, only until recently, undertaken outside of field of health sciences. In contrast, the health sciences (e.g., medicine, nursing, public health) have been, and still are, chiefly oriented towards the biomedical model. They have also been focused on bonding scientific knowledge with the quantification of the elements and variables closest to biology. This characteristic orientation has lead health sciences to overlook the values and behaviors associated with the biographical and social dimensions of the individual (GRACIA, 2000). On the other hand, the weight of the practical component associated with the need to act effectively in the face of illness, disease, and death, as well as the scale of the economic measures and interests involved in treating and preventing them, have also contributed to the frequent sidelining of theoretical and methodological reflections surrounding the complexity of people as subjects and objects of knowledge (MORIN, 1999). [9]
Health-care practices and research need to be linked to science in support of the goals of the greatest benefit and the smallest harm to individuals and populations. This link to science must be understood in the context of its historicity—and thus value-laden—and be open to developing richer and more complete knowledge of this complexity. [10]
For this reason, the development of QHR in both the teaching and research agendas of the healthcare sciences brings with it an especially significant twofold challenge. QHR must be understood and embraced by particular audiences with regard to their original training and professional commitment, and, at the same time, it is to represent not only the acquisition of a set of methods and techniques, but above all it must meet the challenge of a reduced and partial version of scientific knowledge (CALDERÓN & FERNÁNDEZ DE SANMAMED, 2008). [11]
From the theoretical-epistemological point of view, this implies a certain distancing of the field of debate from both the intended positivist "neutrality" of knowledge as well as from some of the most relativistic qualitative trends (SPENCER et al., 2003; MURPHY & DINGWALL, 2003). It also entails a commitment to a form of QHR that is of real use for understanding and improving individual and community health outcomes, and this shall only become feasible when assuming the need for the evaluation of QHR (MORSE, BARRETT, MAYAN, OLSON & SPIERS, 2002). [12]
The special features of quality assessment in the field of QHR as well as their relevance have been reinforced by the prominence attained by "evidence-based" approaches, evidence-based medicine (EBM) being its main exponent. Since its emergence in the 1990's (SACKETT, ROSENBERG, GRAY, HAYNES & RICHARDSON, 1996), the influence of EBM has grown exponentially with regard to publications, courses, handbooks, and clinical practice guidelines. This fact does not, by itself, guarantee the validity of the assumptions of EBM (BUETOW, UPSHUR, MILES & LOUGHLIN, 2006) but it does reflect its relevant impact on the healthcare field. [13]
The legitimate goal for practices not to be based on simple opinions, habits, or different power struggles, explains, to a large extent, the justification and appeal of EBM for many healthcare professionals committed to good clinical practice. However, the frequent drift of EBM development towards reductionist positions, bonding scientific evidence with experimental design has brought with it a significant amount of criticism (ARMSTRONG, 1996; MILES, GREY, POLYCHRONIS, PRICE & MELCHIORRI, 2003; UPSHUR & TRACY, 2004; GRYPDONCK, 2006; KVALE, 2008). This drift has also helped to construct alternative evidence-developing proposals based on approaches including and integrating dimensions and features inherent to QHR (GREENHALGH, 1996; POPAY & WILLIAMS, 1998; BARBOUR, 2000; CONDE, 2001; UPSHUR, 2001). [14]
The implications of EBM for quality assessment in QHR have been notorious. On the one hand, emphasis on systematic reviews and critical appraisal of information on health-care journals and the pharmaceutical industry's "propaganda" has provided a spur for justifying and evaluating the ways in which "qualitative evidence" is constructed; this is how the information is generated and analyzed, and how the results are extracted in the case of QHR. On the other hand, demands for scientific rigor have often reproduced the standardized protocols for reviewing experimental studies in the form of "checklists" or "guidelines," focused on the more technical or procedural aspects; thus, somehow overlooking the substantive or identity elements of QHR (BARBOUR, 2001; EAKIN & MYKHALOVSKIY, 2003). [15]
Recent attempts to synthesize QHR results have also highlighted the need to work on shared instruments for assessing the quality of those results (POPAY, ROGERS & WILLIAMS, 1998; MAYS, POPE & POPAY, 2005; MAHTANI, AXPE, SERRANO, GONZÁLEZ & FERNÁNDEZ, 2006). In these cases the importance of not being reduced to a mere formal echo of a quantitative meta-analysis has been again underlined (BARBOUR & BARBOUR, 2003; SANDELOWSKI & BARROSO, 2007). [16]
I also consider that both components—methodological and substantive—are fundamental to the quality assessment of QHR. As shown in Figure 1, these components can be visually represented by the perpendicular intercept of the two "attracting" axes (CALDERÓN, FERNÁNDEZ DE SANMAMED & BALAGUÉ, 2007). The vertical axis would represent the quality requirements oriented towards methodological rigor and linked to what authors, such as SEALE (2004), have defined as "inner" dialogue. The horizontal axis would correspond to the essential work of discovery and theory development inherent in QHR (SANDELOWSKI & BARROSO, 2003). The quadrant resulting from the effect of both "attracting" axes would represent the area where quality QHR would be situated, and therefore, the area where the methodological proposals aimed at its assessment should be formulated. Should we move away from methodological rigor we would soon find ourselves merely speculating. Should we overlook the substantive components of QR, we could find ourselves mired in formalism of "rigor mortis" (SANDELOWSKI, 1993) or "methodolatry" (CHAMBERLAIN, 2000).
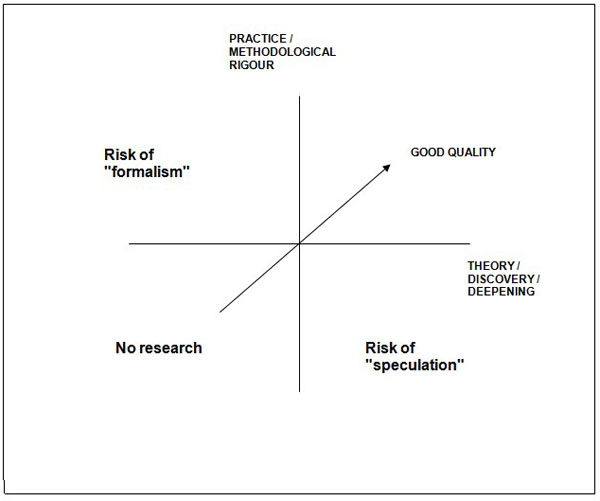
Figure 1: "Attracting"axes and the quality area (CALDERÓN, FERNÁNDEZ DE SANMAMED & BALAGUÉ, 2007) [17]
3. Criteria, Process and Writing
Once the coordinates of a possible area of consensus in the field of QHR quality assessment have been outlined, we now find it appropriate to focus attention on three dimensions present in the assessment process. Despite being necessarily inter-related, these three dimensions should be considered different for the discussion and elaboration of future proposals. [18]
The first of these dimensions represents to the so-called quality criteria. From the very earliest discussions regarding QHR assessment, the debate surrounding the criteria to be followed has been taking place. The majority of these initiatives have agreed upon highlighting the characteristics inherent in QHR as a research methodology, while bearing in mind the influence of the various theoretical approaches referred to earlier in this paper (EMDEN & SANDELOWSKI, 1998; MURPHY et al., 1998; THORNE, 2001). The list of proposals is therefore rather long, ranging from the reproduction of LINCOLN and GUBA's original criteria (1985)—credibility, transferability, dependability and confirmability—(PLA, 1999), to the development of more novel terms and definitions such as those summarized by WHITTEMORE, CHASE & MANDLE (2001): authenticity, explicitness, creativity, vividness, thoroughness, sensitivity, etc. [19]
In my opinion, it is not a matter of terms but rather of content. Criteria should reflect the theoretical-methodological framework of QHR in such a way that they could be used as a point of reference for making decisions concerning the design and procedure of the research process itself, and so for evaluating those decisions as well. It is therefore necessary to underline the importance of discussing the theoretical-methodological content of the criteria, moving beyond generic terms as "goodness" (EMDEN & SANDELOWSKI, 1999), and feeling no fear regarding traditional terms such as validity or relevance (HAMMERSLEY, 1990; FRANKEL, 1999; MALTERUD, 2001). [20]
In this sense, based on four main criteria, I have developed a flexible and open integration of previously published attempts. Those four criteria are epistemological and methodological adequacy, relevance, validity and reflexivity (CALDERÓN, 2002) I shall now briefly introduce them. [21]
The criterion of epistemological and methodological adequacy is the first and foremost requirement when assessing QHR and has been previously discussed by many authors under various names and formats. According to this criterion, before assessing the ways in which information was obtained and analyzed, and results presented, we must first consider what is being studied, whether the qualitative perspective best fits the question and the research objectives, and whether the research design and development as a whole respond to this methodology. The need for this adequacy requires underlining the importance of theory in research along with a two-way assessment process that considers both the totality and its parts, and assesses the degree of coherence between the initial theoretical assumptions and the research work as a whole. [22]
The criterion of relevance has also been acknowledged by numerous authors and should be considered from at least two different standpoints. On the one hand, relevance should be assessed with regard to the pertinence and novelty of the contributions of the research work to the understanding of the phenomenon under study and its implications for the agents involved. On the other hand, relevance should be evaluated in relation to the implications of the research results beyond the specific circumstances in which the work has been developed. The response to this unease, which LINCOLN and GUBA (1985) have termed "transferability," is not guided, in the case of QHR, by statistical patterns but rather depends on the degree of abstraction/depth attained when interpreting the phenomenon, and also on the thoroughness of the description of the circumstances under which the research work was conducted. As I will discuss in more detail below, the generalization of QHR results is necessarily linked to the development of the other criteria. Thus, considering it a central referent point for quality rating (DALY et al., 2007) can generate confusion with regard to the role to be played by each of the other criteria. [23]
The criterion of validity is also essential for QHR. Several authors' definitions of the concept encompass some of the requirements that I have placed under separate criteria (WHITTEMORE et al., 2001; MAXWELL, 2005). From my point of view, validity responds, first of all, to a commitment to fidelity to the actual behavior of the phenomenon under study, which requires maximum rigor in the study design as well as during data collection and validation. At the same time, validity in QHR should focus on its interpretive analytical features, as previously expressed in terms of "plausibility" (KUZEL & LIKE, 1991) or "credibility" (SPENCER et al., 2003). In an attempt to highlight the importance of trying to make the audiences feel like active participants in the creative interpretive process undertaken on the basis of the empirical work, I have named this component "interpretive complicity" (CALDERÓN, 2007). [24]
Considering reflexivity as a criterion responds to the key nature of this concept for social research in general, and for QHR in particular (HAMMERSLEY & ATKINSON, 1983; MALTERUD, 2001), as it represents researchers' self-awareness of their own theoretical assumptions and perspectives in relation to the design of the study, relationships with participants, and the development of the study as a whole. The non-concealment of researchers (ALONSO, 1998; BARKER & PISTRANG, 2005) also allows for a closer assessment of their "responsiveness" (MORSE et al., 2002) and for underlining the need to consider ethical aspects as fundamental components of QHR assessment, not only in the development of the study (GUILLEMIN & GILLAM, 2004; BARRIO-CANTALEJO & SIMÓN-LORDA, 2006) but also when justifying it and when transferring its results to practice. [25]
These criteria are involved in the dynamic and circularity of QHR in such a way that their mutual interaction and overlap are constant issues in the assessment process. The relevance of the research work will, to a large extent, depending on its validity. Applying validity requires exercising reflexivity, along with assuming its subsequent ethical demands. Furthermore, the research work as a whole should respond to the methodological adequacy of QHR as a distinct "gaze" or knowledge perspective. [26]
Going beyond suitability when formulating the aforementioned criteria—which is obviously open to discussion—it is now of particular interest to highlight the importance of differentiating these criteria as a dimension of its own in the quality assessment of QHR. As discussed earlier, these criteria become absolutely necessary when linking the assessment of the quality to the theoretical-methodological features of QHR. Thus, their guiding role is located at a level that is both previous and different to that of the evaluation of the steps taken at each phase of the research process. Consequently, criteria should be visually placed at the base, or initial zone, of the quadrant representing the "quality area" (Figure 2).
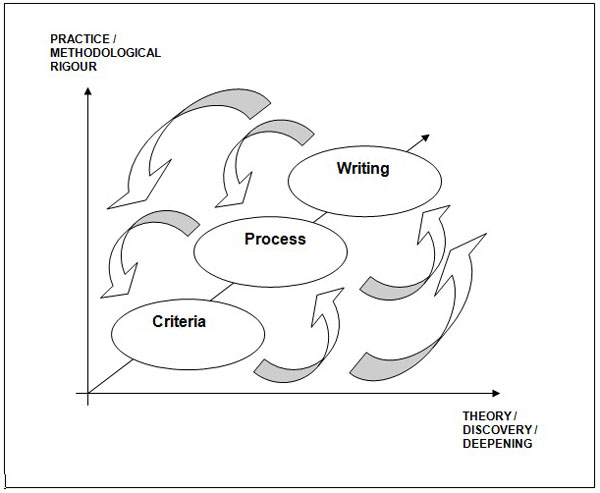
Figure 2: Dimensions of quality assessment [27]
Once the function and level of intervention of the criteria are determined, I agree with authors such as MORSE et al. (2002) and SEALE (2004) who underline the importance of considering QHR as a dynamic process in which quality has to be generated at each and every step of the research process. As we already know, this practice never actually unfolds in a linear way but rather behaves in a very flexible and iterative way, holding permanent overlaps between its different phases. Consequently, the need is now soundly justified to evaluate the development of each one of these phases or moments (definition and justification of the question and research objectives, literature search and support, design, selection of information sources and generation techniques, analysis and discussion of results) making explicit the recommendations to be fulfilled at each step (ELDER & MILLER, 1995; FRANKEL, 1999; SPENCER et al., 2003; GREENHALGH, 2006; CRESWELL, 2007; FLICK, 2007). [28]
Such evaluative work also influences validation and improvement techniques and procedures being used in the research process (e.g. triangulation, "member checking," detailed description of interventions), shaping a differentiated dimension of quality assessment that, for being sustained in the research process, we have decided to name as such. In this case, the evaluative work requires particular norms and guidance strategies that are adequate to each phase of the process and that we can find thoroughly described in most of the critical evaluation guides (FERNÁNDEZ DE SANMAMED, 2000; GIACOMINI & COOK, 2000; BLAXTER, 2000; SANDELOWSKI & BARROSO, 2002; BROMLEY et al., 2002; GREENHALGH, 2006). I have attempted to summarize the most important proposals in the central column in Figure 3 and will come back to them later in this paper. [29]
The link between the dimensions related to the criteria and the process is permanent in such a way that the understanding and appropriate use of the rules associated with the process are only possible if the theoretical-methodological reference of the criteria that justify and give sense to them is kept in sight. I thus consider it inappropriate to focus the attention of quality assessment on the quality of those rules or requirements (DIXON-WOODS, SHAW & SMITH, 2004; BERGMAN & COXON, 2007; KUPER, LINGARD & LEVINSON, 2008), or to suggest locating them at the same level as the criteria (MAYS & POPE, 2000). [30]
The visual representation of the process-related requirements would have them on a layer at the back of the emerging picture (Figure 2). [31]
Finally, we must consider the writing dimension, defined as the graphic expression of the research work, usually in the form of a report or an article. Elaborating and disseminating the research work can be considered the final phase in the QHR process, but it nevertheless holds certain features justifying their differentiation in QR quality assessment. [32]
Writing constitutes the re-presentation of the research work, and therefore every main component of this process, theoretical as well as methodological, from justification of the research question and objectives to the discussion of results and conclusions, should be considered when elaborating and evaluating it. In this sense, questions regarding the development of each one of the phases or moments in the research process become, in this case, equally pertinent and necessary. In fact, these questions are present in almost all the critical appraisal proposals mentioned earlier, whether in the form of guides or "checklists." [33]
As such re-presentation writing cannot be understood without taking into account its rhetorical component and its target audience (SANDELOWSKI & BARROSO, 2002; GOLDEN-BIDDLE & LOCKE, 2007). Whether in the form of a report, an article, or an oral presentation, writing is always developed bearing a specific target audience in mind. While sometimes this target represents the final intended audience itself, most of the time it is the editorial board of the journal or institution, with their respective reviewers and pre-established formats that constitute that first audience of our writing. [34]
In either case, writing entails certain quality requirements aimed at achieving a successful dialogue (SANDELOWSKI, 1998), in addition to spatial and stylistic requirements that can often conceal and distort the actual content of the research. The "scientific format" required by the majority of journals determines the representation of the research process by fragmenting it and reducing it to previously designed spaces. Similarly, the author is often asked to use an impersonal linguistic style that does not represent his or her involvement in the research process. It is nevertheless also true that sometimes it is the author or researcher who takes advantage of the "seductive power of words" (DALY et al., 2007) and uses it to conceal the weaknesses in the content of the presentation. [35]
Thus, writing in QHR requires special attention in the assessment process, a process that will have to consider the ways in which communication between the audience and the content is facilitated, and the ways in which this content is assessed beyond the artificial nature of the different formats. Its visual representation would therefore necessarily link it to the research process it intends to represent, but would place it at a more "peripheral" location (Figure 2). [36]
4. Relationship Between Dynamics and Levels in QHR Quality Assessment
The QHR quality assessment process must respond to the dynamic, flexible, and circular behavior inherent to this research methodology, closely mirroring the attitudes and abilities displayed by the researcher when undertaking his or her work. The permanent going back and forth between the general and the specific that takes place once the research question as been defined, as well as when selecting, generating, and analyzing the information, also occurs during assessment. Furthermore, the overlap between the different phases or moments of the research process also takes place in the assessment process as the dimensions of criteria, process, and writing interrelate in such a way that their reciprocal correspondence should never be understood as one-way or linear. [37]
As I have previously outlined the case of systematic reviews in QHR (CALDERÓN, 2004), I think it would be feasible to incorporate the three assessment levels mentioned earlier into a common scheme, aiming at better understanding the nature of their relationship (Figure 3). I present the quality criteria in the first column, the particular requirements or questions to be taken into account during the different phases of the research process in the second one, and the sections into which the writing of the research is normally structured in a publishable or published research paper in the third column.
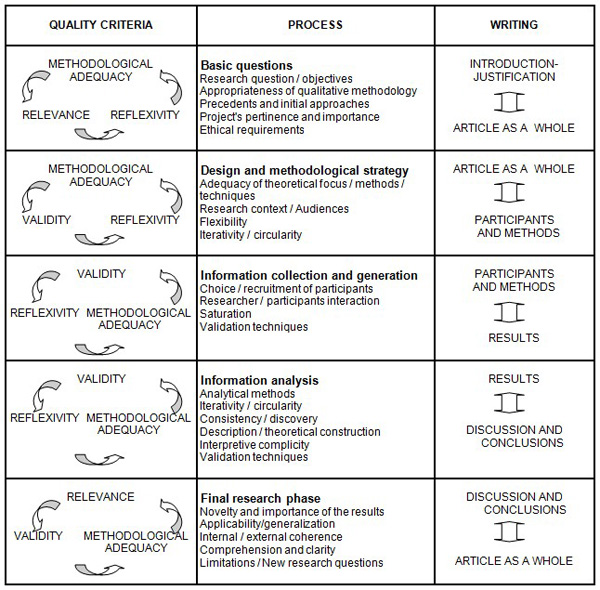
Figure 3: Dimensions of quality assessment in QHR [38]
Thus, should we start from the basic questions of the qualitative research process, the first column, criteria would show us their correspondence to methodological adequacy (correspondence with the theoretical approach and the research question), and also to relevance (novel and pertinent findings) and reflexivity (role of the researcher/ethics), with their inherent inter-relationships and overlaps. Should we attempt to place the responses to those basic questions in the writing dimension, we would need to focus our search on the Introduction/Justification section, but also in the reading of the article as a whole. [39]
Framing the design and methodological strategy in the planning phase of the research process also sets certain requirements for which methodological adequacy and reflexivity remain as key reference criteria, along with validity, particularly with regard to rigor and transparency. In the writing dimension, it would be through the assessment of the section on Participants and methods as well as of the article as a whole where we should focus our critical appraisal. [40]
The information collection and generation phase entails actual work on the ground, and thus requires the analysis of issues more closely related to methods and procedures. Although each holding different levels of prominence, validity, reflexivity, and methodological adequacy will again be the main quality criteria to be considered, while keeping the discovery component I previously introduced when exploring relevance. Sections on Participants and methods and Results would now be the main sites for the writing dimension. [41]
I have previously pointed out the correspondence between the dynamics of research and assessment processes, but it could be appropriate to recall it when talking about analysis in QHR. Each analytical method (thematic analysis, content analysis, grounded theory, conversational analysis, discourse analysis, etc.) entails its own features when working with the texts and the contexts in which they were generated. Each method of analysis also places a different emphasis on the interpretive component, which necessarily influences the focus of the quality assessment. This is why it becomes important to first of all, reflect upon the analytical model chosen and the steps taken during the process. When assessing quality at this analytical phase we also assess circularity and iterativity both in relation to the previous information-generation phase, and to the going back and forth from the level of empirical data to the more theoretical level represented by the results. Despite the risk of excessive schematization when considering all different analytical methods together, validity, understood both as rigor and interpretive power, will in this case be the quality criterion justifying, to a larger extent, the questions and issues related to this phase, along with reflexivity and methodological adequacy. This time, the sections on Results and Discussion and conclusions, either together or as different sections, constitute interest in the writing dimension. [42]
When reaching the final research phase, questions for which relevance is again of particular importance as a criterion are required, along with validity and, of course, methodological adequacy in its—now retrospective—aspects of coherence between the design and the implementation of the research work. Back to the writing dimension, although it is true that the Discussion and conclusions make up the final field of the research work, quality assessment will be difficult to conduct if not taking the article as a whole into consideration. [43]
In short, quality assessment in QHR should not be understood as a rigid process, nor should it be reduced to a dichotomy of the presence or absence of a requirement or procedure in a particular section of the article or report to be assessed. This is why I insist on highlighting the dynamic and interactive nature of the relationship between the different dimensions and their main components. This nature of the process also calls for caution when using checklists supported through quantification methods or software applications (KMET, LEE & COOK, 2004; PEARSON, 2004) aimed at facilitating the necessarily difficult assessment process, as it requires an integrative and dynamic perspective on the dimensions analyzed as a whole. [44]
QR quality assessment should be coherent with the particular features of that research methodology and the particularities of the contexts, objects, and agents involved in its practice. In this respect, health and healthcare fields need areas of consensus that favor QHR integration in an open-to-human-complexity scientific space. Quality of QHR represents an essential requirement for that integration but also for what should certainly become its commitment to the improvement of individual and community health and healthcare provision. [45]
From these assumptions, the demarcation of an area of debate responding to the "substantive" theoretical-methodological components of QHR and to the rigor requirements of the research work is justified, and the differentiation of those three dimensions related to criteria, process, and writing in quality assessment of QHR is soundly sustained. [46]
Each of these three dimensions supports differentiated, although mutually interrelated, functions in the evaluative work. Criteria represent the necessary link of such work with the singularity of QHR as a research methodology, and thus constitute its baseline reference. Attempting to synthesize other authors' previous contributions, methodological and epistemological adequacy, relevance, validity and reflexivity criteria have been described, and the iterativity and overlapping of their interactions acknowledged. The so-called process dimension includes the set of validation and quality improvement requirements and procedures to be considered through the practical implementation of the research process. Its formulation should run along the different phases of that process, also incorporating contributions coming from the numerous guides and lists previously published. Finally, writing as a differentiated and more peripheral dimension of quality assessment underlines the importance of dialoguing with audiences and the need to consider both the contents as well as the rhetorical components, including the limits emerging from the artificially constructed nature of the formats. [47]
The dynamic interrelation between the three dimensions has been especially highlighted and graphically represented by means of a common table. This table integrates the role of quality criteria, the most important aspects to be taken into account when evaluating the research process, and the different sections usually considered when writing the research. [48]
These proposals are undoubtedly open to discussion and development, both theoretical and methodological. As I have tried to convey through this paper, it is not a matter of claiming uniform checklists or guidelines, but rather defining common areas of work and debate in the field of quality assessment of QHR. To my understanding, instrumental plurality, flexibility, and discovery inherent in QHR should also be compatible with the approach and consensus I am calling for. [49]
The author would like to sincerely thank Amaia Sáenz de ORMIJANA for her comments and help on the English version of this paper, as well as BIOEF (Basque Foundation for Health Innovation and Research).
Alonso, Luis Enrique (1998). La mirada cualitativa en sociología. Una aproximación interpretativa. Madrid: Editorial Fundamentos.
Armstrong, David (1996). Measuring man: Some problems of method. Family Practice, 13(Suppl.1), 6-9.
Atkinson, Paul (1995). Some perils of paradigms. Qualitative Health Research, 5, 117-124.
Barbour, Rosaline S. (2000). The role of qualitative research in broadening the "evidence base" for clinical practice. Journal of Evaluation in Clinical Practice, 6, 155-163.
Barbour, Rosaline S. (2001). Checklists for improving rigour in qualitative research: A case of the tail wagging the dog? British Medical Journal, 322, 1115-1117.
Barbour, Rosaline S. & Barbour, Michael (2003). Evaluating and synthesizing qualitative research: The need to develop a distinctive approach. Journal of Evaluation in Clinical Practice, 9, 179-186.
Barker, Chris & Pistrang, Nancy (2005). Quality criteria under methodological pluralism: Implications for conducting and evaluating research. American Journal of Community Psychology, 35, 201-212.
Barrio-Cantalejo, Inés M. & Simón-Lorda, Pablo (2006). Problemas éticos de la investigación cualitativa. Medicina Clínica (Barcelona), 126, 418-423.
Beltrán, Miguel (1986). Cuestiones previas acerca de la ciencia de la realidad social. In Manuel García F., Jesús Ibáñez & Francisco Alvira (Eds.), El análisis de la realidad social. Métodos y técnicas de investigación (pp.17-29). Madrid: Alianza Editorial SA.
Bergman, Manfred Max & Coxon, Anthony P. M. (2007). The quality in qualitative methods. Forum Qualitative Sozialforschung / Forum: Qualitative Social Research, 6(2), Art. 34, http://nbn-resolving.de/urn:nbn:de:0114-fqs0502344 [Date of access: 01, 12, 2007].
Blaxter, Mildred (2000). Criteria for qualitative research. Medical Sociology News, 26, 34-37.
Bromley, Helen; Dockery, Grindi; Fenton, Carrie; Nhlema, Bertha; Smith, Helen; Tolhurst, Rachel & Theobald, Sally (2002). Criteria for evaluating qualitative studies. Liverpool: Liverpool School of Tropical Medicine.
Buetow, Stephen; Upshur, Ross; Miles, Andrew & Loughlin, Michael (2006). Taking stock of evidence-based medicine: Opportunities for its continuing evolution. Journal of Evaluation in Clinical Practice, 12, 399-404.
Calderón, Carlos (2002). Criterios de calidad en la Investigación Cualitativa en Salud (ICS): Apuntes para un debate necesario. Revista Española de Salud Pública, 76, 473-482.
Calderón, Carlos (2004). Las revisiones sistemáticas y el reto de la evaluación de la calidad en la investigación cualitativa en salud. Atención Primaria, 34, 166-169.
Calderón, Carlos (2007). Evaluación y presentación de la investigación cualitativa. In Carlos Calderón, Fernando Conde, María José Fernández de Sanmamed & Olga Monistrol (Eds.), Curso de introducción a la investigación cualitativa. Máster de investigación en atención primaria (pp.1-43). Barcelona: semFYC, Universitat Autònoma de Barcelona, Fundació Doctor Robert.
Calderón, Carlos & Fernández de Sanmamed, María José (2008). Investigación cualitativa en atención primaria. In A. Martín Zurro & J.F. Cano Pérez (Eds.), Atención primaria. Conceptos, organización y práctica clínica (6th ed., pp.211-240). Barcelona: Elsevier.
Calderón, Carlos; Fernández de Sanmamed, María José & Balagué, Laura (2007, May). Quality and critical appraisal in qualitative health research: Discussion of an integrative proposal. Paper presented at the Third International Congress of Qualitative Inquiry, Urbana-Champaign, USA.
Chamberlain, Kerry (2000). Methodolatry and qualitative health research. Journal of Health Psychology, 5, 285-296.
Chapple, Alison & Rogers, Anne (1998). Explicit guidelines for qualitative research: A step in the right direction, a defence of the "soft" option, or a form of sociological imperialism? Family Practice, 15, 556-561.
Conde, Fernando (2001). La investigación cualitativa en salud desde la perspectiva histórico-sociológica. Atención Primaria, 28(Suppl.1), 199-200.
Conde, Fernando (2002). Encuentros y desencuentros entre la perspectiva cualitativa y la cuantitativa en la Historia de la Medicina. Revista Española de Salud Pública, 76, 395-408.
Creswell, John W. (2007). Qualitative inquiry and research design. Choosing among five approaches (2nd ed.). Thousand Oaks, CA: Sage.
Daly, Jeanne; Willis, Karen; Small, Rhonda; Green, Julie; Welch, Nicky; Keally, Michelle & Hughes, Emma (2007). A hierarchy of evidence for assessing qualitative health research. Journal of Clinical Epidemiology, 60, 43-49.
De Souza Minayo, María Cecilia (1995). El desafío del conocimiento. Buenos Aires: Lugar Editorial.
Denzin, Norman K. & Lincoln, Yvonna S. (1994). Entering the field of qualitative research. In Norman K. Denzin & Yvonna S. Lincoln (Eds.), Handbook of qualitative research (pp.1-17). Thousand Oaks, CA: Sage.
Denzin, Norman K. & Lincoln, Yvonna S. (2005). Introduction: The discipline and practice of qualitative research. In Norman K. Denzin & Yvonna S. Lincoln (Eds.), The Sage handbook of qualitative research (3rd ed., pp.1-32). Thousand Oaks, CA: Sage.
Dixon-Woods, Mary; Shaw, Rachel L. & Smith, Jonathan A. (2004). The problem of appraising qualitative research. Quality and Safety in Health Care, 13, 223-225.
Eakin, Joan M. & Mykhalovskiy, Eric (2003). Reframing the evaluation of qualitative research: Reflections on a review of appraisal guidelines in the health sciences. Journal of Evaluation in Clinical Practice, 9, 187-194.
Elder, Nancy C. & Miller, William L. (1995). Reading and evaluating qualitative research studies. The Journal of Family Practice, 41, 279-285.
Emden, Carolyn & Sandelowski, Margarete (1998). The good, the bad and the relative, part one: Conceptions of goodness in qualitative research. International Journal of Nursing Practice, 4, 206-212.
Emden, Carolyn & Sandelowski, Margarete (1999). The good, the bad and the relative, part two: Goodness and the criterion problem in qualitative research. International Journal of Nursing Practice, 5, 2-7.
Fernández de Sanmamed, María José (2000). Adecuación de las normas de publicación en revistas científicas a las investigaciones cualitativas. Atención Primaria, 25, 502-504.
Flick, Uwe (2007). Managing quality in qualitative research. London: Sage.
Frankel, Richard M. (1999). Standards of qualitative research. In Benjamin F. Crabtree & William L. Miller (Eds.), Doing qualitative research (2nd ed., pp.333-346). Thousand Oaks, CA: Sage.
Giacomini, Mita K. & Cook, Deborah J. for the Evidence-Based Medicine Working Group (2000). Users' guides to the medical literature. XXIII. Qualitative research in health care. A. Are the results of the study valid? Journal of the American Medical Association, 284, 357-362.
Golden-Biddle, Karen & Locke, Karen (2007). Composing qualitative research. Thousand Oaks, CA: Sage.
Gracia, Diego (2000). El futuro del nuevo modelo de relación clínica. Dimensión Humana, 4, 3.
Greenhalgh, Trisha (1996). "Is my practice evidence-based?": Should be answered in qualitative, as well as quantitative terms. British Medical Journal, 313, 957-958.
Greenhalgh, Trisha (2006). Papers that go beyond numbers (qualitative research). In Trisha Greenhalgh (Ed.), How to read a paper. The basis of evidence-based medicine (3rd ed., pp.166-179). Oxford: Blackwell.
Grypdonck, Mieke H. (2006). Qualitative health research in the era of evidence-based practice. Qualitative Health Research, 16, 1371-1385.
Guba, Egon G. & Lincoln, Yvonna S. (2005). Paradigmatic controversies, contradictions, and emerging confluences. In Norman K. Denzin & Yvonna S. Lincoln (Eds.), The Sage handbook of qualitative research (3rd ed., pp.191-215). Thousand Oaks, CA: Sage.
Guillemin, Marilys & Gillam, Lynn (2004). Ethics, reflexivity, and "ethically important moments" in research. Qualitative Inquiry, 10, 261-280.
Hammersley, Martyn (1990). Reading ethnographic research. New York: Longman.
Hammersley, Martyn & Atkinson, Paul (1983). Ethnography: Principles in practice. London: Routledge.
Íñiguez, Lupicinio (1999). Investigación y evaluación cualitativa: Bases teóricas y conceptuales. Atención Primaria, 23, 496-502.
Kmet, Leanne M.; Lee, Robert C. & Cook, Linda S. (2004). Standard quality assessment criteria for evaluating primary research papers from a variety of fields. Edmonton: AHFMR.
Kuper, Ayelet; Lingard, Lorelei & Levinson, Wendy (2008). Critically appraising qualitative research. British Medical Journal, 337, a1035.
Kuzel, Anton J. & Like, Robert C. (1991). Standards of trustworthiness for qualitative studies in primary care. In Peter G. Norton, Moira Stewart, Fred Tudiver, Martin J. Bass & Earl V. Dunn (Eds.), Primary care research: Traditional and innovative approaches (pp.138-158). Newbury Park, CA: Sage.
Kvale, Steinar (2008). Qualitative inquiry between scientistic evidentialism, ethical subjectivism and the free market. International Review of Qualitative Research, 1, 5-18.
Leys, Mark (2003). Health care policy: Qualitative evidence and health technology assessment. Health Policy, 65, 217-226.
Lincoln, Yvonna S. & Guba, Egon G. (1985). Naturalistic inquiry. Newbury Park, CA: Sage.
Mahtani, Vinita; Axpe, María Ángeles; Serrano, Pedro; González, Inmaculada & Fernández, Enrique (2006). Metodología para incorporar los estudios cualitativos en la evaluación de tecnologías sanitarias. Madrid: Plan Nacional para el SNS del MSC, Servicio de Evaluación del Servicio Canario de Salud.
Malterud, Kirsti (2001). Qualitative research: Standards, challenges, and guidelines. Lancet, 358, 483-488.
Maxwell, Joseph A. (2005). Qualitative research design. An interactive approach (2nd ed.). Thousand Oaks, CA: Sage.
Mays, Nicholas & Pope, Catherine (2000). Assessing quality in qualitative research. British Medical Journal, 320, 50-52.
Mays, Nicholas; Pope, Catherine & Popay, Jennie (2005). Systematically reviewing qualitative and quantitative evidence to inform management and policy-making in the health field. Journal of Health Services Research and Policy, 10(Suppl.1), 6-20.
Mercado, Francisco J.; Lizardi, Alejandra & Villaseñor, Martha (2002). Investigación cualitativa (en salud) en América Latina. Una aproximación. In Francisco J. Mercado, Denise Gastaldo & Carlos Calderón (Eds.), Paradigmas y diseños en Investigación Cualitativa en Salud. Una Antología Iberoamericana (I) (pp.133-157). Guadalajara: Universidad de Guadalajara, Universidad Autónoma de Nuevo León, Servicio Vasco de Salud-Osakidetza, Asociación Médica de Jalisco, Instituto Jalisciense de Cancerología.
Miles, Andrew; Grey, Joseph E.; Polychronis, Andreas; Price, Nicholas & Melchiorri, Claudio (2003). Current thinking in the evidence-based health care debate. Journal of Evaluation in Clinical Practice, 9, 95-109.
Morin, Edgar (1999). Los principios de un conocimiento pertinente. In Edgar Morin (Ed.), Los siete saberes necesarios para la educación del futuro (pp.14-20). París: Organización de las Naciones Unidas para la Educación, la Ciencia y la Cultura, UNESCO.
Morse, Janice M. (1994). Critical issues in qualitative research methods. Thousand Oaks, CA: Sage.
Morse, Janice M. (2007a). What is the domain of qualitative health research? Qualitative Health Research, 17, 715-717.
Morse, Janice M. (2007b). Does health research warrant the modification of qualitative methods? Qualitative Health Research, 17, 863-865.
Morse, Janice M.; Barrett, Michael; Mayan, Maria; Olson, Karin & Spiers, Jude (2002). Verification strategies for establishing reliability and validity in qualitative research. International Journal of Qualitative Methods, 1, Art. 2, http://www.ualberta.ca/~iiqm/backissues/1_2Final/html/morse.html [Data of access: 07, 10, 2003].
Murphy, Elizabeth & Dingwall, Robert (2003). Qualitative methods and health policy research. New York: Aldine de Gruyter.
Murphy, Elizabeth; Dingwall, Robert; Greatbatch, David; Parker, Susan & Watson, Pamela (1998). Qualitative research methods in health technology assessment: A review of the literature. Health Technology Assessment, 2(16), http://www.hta.ac.uk/fullmono/mon216.pdf [Data of access: 24, 03, 2000].
Patton, Michael Q. (2002). Enhancing the quality and credibility of qualitative analysis. In Michael Q. Patton (Ed.), Qualitative research and evaluation methods (3rd ed., pp.541-588). Thousand Oaks, CA: Sage.
Pearson, Alan (2004). Balancing the evidence: Incorporating the synthesis of qualitative data into systematic reviews. Joanna Briggs Institute Reports, 2, 45-64.
Pla, Margarida (1999). El rigor en la investigación cualitativa. Atención Primaria, 24, 295-300.
Popay, Jennie & Williams, Gareth (1998). Qualitative research and evidence-based health care. Journal of the Royal Society of Medicine, 91, 32-37.
Popay, Jennie; Rogers, Anne & Williams, Gareth (1998). Rationale and standards for the systematic review of qualitative literature in health services research. Qualitative Health Research, 8, 341-351.
Ratcliffe, John W. & González del Valle, Amalia (2000). El rigor en la investigación de la salud: Hacia un desarrollo conceptual. In Catalina A. Denman & Jesús A. Haro (Eds.), Por los rincones: Antología de métodos cualitativos en la investigación social (pp.57-111). Hermosillo: El Colegio de Sonora.
Rodríguez, Gregorio; Gil, Javier & García, Eduardo (1996). Metodología de la investigación cualitativa. Archidona: Ediciones Aljibe.
Sackett, David L.; Rosenberg, William M.C.; Gray, J.A. Muir; Haynes, R. Brian & Richardson, W. Scott (1996). Evidence based medicine: What it is and what it isn't. British Medical Journal, 312, 71-72.
Sandelowski, Margarete (1993). Rigor or rigor mortis: The problem of rigor in qualitative research revisited. Advances in Nursing Science, 16, 1-8.
Sandelowski, Margarete (1998). Writing a good read: Strategies for re-presenting qualitative data. Research in Nursing and Health, 21, 375-382.
Sandelowski, Margarete & Barroso, Julie (2002). Reading qualitative studies. International Journal of Qualitative Methods, 1(1), 74-108, https://ejournals.library.ualberta.ca/index.php/IJQM/article/view/4615/3764 [Data of access: 14, 02, 2003].
Sandelowski, Margarete & Barroso, Julie (2003). Classifying the findings in qualitative studies. Qualitative Health Research, 13, 905-923.
Sandelowski, Margarete & Barroso, Julie (2007). Handbook for synthesizing qualitative research. New York: Springer.
Seale, Clive (2004). Quality in qualitative research. In Clive Seale, Giampietro Gobo, Jaber F. Gubrium & David Silverman (Eds.), Qualitative research practice (pp. 409-419). London: Sage.
Smith, John K. & Deemer, Deborah K. (2000). The problem of criteria in the age of relativism. In Norman K. Denzin & Yvonna S. Lincoln (Eds.), Handbook of qualitative research (2nd ed., pp.877-896). Thousand Oaks, CA: Sage.
Spencer, Liz; Ritchie, Jane; Lewis, Jane; Dillon, Lucy & National Centre for Social Research (2003). Quality in qualitative evaluation: A framework for assessing research evidence, http://www.gsr.gov.uk/downloads/evaluating_policy/a_quality_framework.pdf [Data of access: 19, 02, 2004].
Thorne, Sally E. (2001). The implications of disciplinary agenda on quality criteria for qualitative research. In Janice M. Morse, Janice M. Swanson & Anton J. Kuzel (Eds.), The nature of qualitative evidence (pp.141-159). Thousand Oaks, CA: Sage.
Ulin, Priscilla R.; Robinson, Elizabeth T. & Tolley, Elizabeth E. (2005). Qualitative methods in public health. A Field guide for applied research. San Francisco: Jossey-Bass.
Upshur, Ross E.G. (2001). The status of qualitative research as evidence. In Janice M. Morse, Janice M. Swanson, & Anton J. Kuzel (Eds.), The nature of qualitative evidence (pp.5-26). Thousand Oaks, CA: Sage.
Upshur, Ross E.G. & Tracy, C. Shawn (2004). Legitimacy, authority and hierarchy: Critical challenges for evidence-based medicine. Brief Treatment and Crisis Intervention, 4, 197-204.
Vallés, Miguel (1997). Técnicas cualitativas de investigación social. Reflexión metodológica y práctica profesional. Madrid: Síntesis SA.
Vasilachis de Gialdino, Irene (2006). La investigación cualitativa. En Irene Vasilachis de Gialdino (Ed.), Estrategias de investigación cualitativa (pp.23-64). Barcelona: Gedisa.
Whittemore, Robin; Chase, Susan K. & Mandle, Carol L. (2001). Validity in qualitative research. Qualitative Health Research, 11, 522-537.
Carlos CALDERÓN GÓMEZ, PhD, MD (Family and Community Medicine Specialist), MA Sociology, MPH.
Presently, Carlos CALDERÓN works as a Family Doctor and Trainer of Family and Community Medicine Residents in the Basque Health Service-Osakidetza's Health Centre in Alza (San Sebastian). He has participated in teaching Family Medicine since its beginnings in the Basque Country, and has worked as a Visiting Research Fellow at the Centre for Health Services Research of the University of Newcastle upon Tyne, UK.
Since the early 1990's he has been involved in promoting, teaching, and developing Qualitative Health Research (QHR), with particular emphasis on the field of Primary Health-Care.
He is a member of the Editorial Board of the journals Qualitative Health Research and Atención Primaria, the author of several publications and lecturer in numerous courses and workshops in the field of quality assessment in QHR. He has coordinated the REDICS (Qualitative Health Research Network) project of the Nursing Research Coordination and Development Unit (Investén) at the Carlos III Health Institute since its inception.
Contact:
Carlos Calderón Gómez
Centro de Salud de Alza. Osakidetza-Servicio Vasco de Salud
REDICS-Investén. Instituto de Salud Carlos III
C/ Pasajes, 6, 5º izda
20013 San Sebastián, Spain
Tel.: 943-286934 / 943-006520
Fax: 943-006507
E-mail: ccalderong@telefonica.net, carlos.calderongomez@osakidetza.net
Calderón Gómez, Carlos (2009). Assessing the Quality of Qualitative Health Research: Criteria, Process and Writing [49 paragraphs]. Forum Qualitative Sozialforschung / Forum: Qualitative Social Research, 10(2), Art. 17, http://nbn-resolving.de/urn:nbn:de:0114-fqs0902178.

Creative Commons Attribution 4.0 International License