Volume 21, No. 1, Art. 8 – January 2020
Participatory Health Research With Mothers Living in Poverty in the Netherlands: Pathways and Challenges to Strengthen Empowerment
Barbara C. Groot & Tineke A. Abma
Abstract: Empowerment of people in challenging circumstances is a central premise of participatory health research (PHR). Empowerment, a process of strengthening vis-à-vis one's social environment, has three components: personal, relational, and political. The current PHR study was conducted with mothers living in unfortunate situations in the Netherlands. In this article, we describe how PHR fostered personal empowerment to a certain degree by 1. setting an agenda for the project (ownership), and 2. listening to and acknowledging the articulation of the participants' own story and a collective story about their issues (epistemic justice). One result of the study is that achieving relational and political empowerment can be challenging. Relational tensions in the group distracted us. Conducting critical reflection on more structural causes of the unfortunate situations of the mothers is a process that needs time and calls for relational sensitivity and inclusion. The participatory researcher as facilitator focused on ethics and tried to collaborate with creative outsiders to change the disharmony in the group. Reaching relational and political empowerment is a long-term process in PHR, but not without stumbling blocks on the journey.
Key words: participatory health research; mothers; poverty; relational empowerment; epistemic justice; ethics
Table of Contents
1. Introduction
2. Theoretical Background
3. Objectives and Methodology
3.1 Research setting
3.2 Co-research group
3.3 Participatory health research
3.4 Ways to collaborate with the mothers
3.5 Research ethics
4. Findings
4.1 Personal understanding through storytelling
4.2 Mutual understanding through interactions with stakeholders
4.3 Deepening personal understanding: More creative methods
5. Discussion
6. Conclusion
The central premise of participatory health research (PHR) is to maximize the participation of people in unfortunate situations, strengthen their empowerment, and create social change for social justice. First, the defining principle of PHR is inclusion and democratic participation of those whose life or work is the subject of the research in all stages of the research process (ABMA et al., 2019; ICPHR, 2013a; WRIGHT & KONGATS, 2018). This process includes the full research cycle, starting with the formulation of the research question and goal, development of the research design, selection of appropriate methods for data gathering and analysis, dissemination of the findings, and collaborating and monitoring actions. A second principle of PHR is that people in marginalized positions are heard (ABMA et al., 2019). The intention in PHR is to value all knowledges and experiences. By appraising marginalized voices, active learning, and collective action to solve problems, PHR facilitators aim to empower individuals, communities, and organizations (ibid.). Finally, a third principle of PHR is social change for social justice. The approach of PHR has the explicit goal of creating positive social change by the process of researching with those persons whose life or work is the focus of the research (ibid., see also ICPHR, 2013a; WRIGHT & KONGATS, 2018). [1]
So far, little attention has been paid to detailed descriptions of the processes set in motion through PHR studies (COOK, BOOTE, BUCKLEY, VOUGIOUKALOU & WRIGHT, 2017). We lack insights into the process of developing strength vis-à-vis one's environment by use of PHR. Besides, descriptions about group dynamics in participatory action research groups are also rarely documented (ADILI, HIGGINS & KOCH, 2013). Therefore, we present the first years of the process of a PHR study, titled You Do Not See It with Dutch mothers living in poverty (living on €50,- per month). The process is still going on at the moment of writing this article. The research question addressed in the current article is: What are pathways and challenges to strengthening personal, relational, and political empowerment via PHR, and how can we understand these? [2]
We aim to contribute to a growing area of research on how to conduct PHR in order to foster empowerment processes with marginalized groups in society. We highlight both the relational dynamics in PHR as well as the processes that were focused on fostering empowerment. In line with a tendency among qualitative social researchers (AAMANN, 2017; VITUS, THUESEN & TANGGAARD, 2014), we do not avoid themes as disharmony and conflicts. As VITUS et al. (2014, p.15) state, conflicts are not technical problems caused by using "wrong" methods or by the researcher's inadequate navigation in the field. However, understanding conflicts as they state, is a vital aspect of the epistemological, methodological, and analytical foundation of research. Reflections on conflict and its complexity are unavoidable and a condition for the production of social scientific knowledge. A reflexive process makes PHR more transparent and methodologically and analytically insightful. [3]
The article is organized into four parts. We start with the theoretical background of empowerment (Section 2) and our methodology (Section 3). Then we present a story of the process, including reflections that contain "uncomfortable" reflections (Section 4). These reflections are, as PILLOW (1993, p.193) states, "messy" examples, "examples that may not always be successful, examples that do not seek a comfortable, transcendent end-point but leave us in the uncomfortable realities of doing engaged qualitative research." We included these reflections, because according to PILLOW, the qualitative research arena would benefit from uncomfortable reflexivity. Finally, we end with a discussion about empowerment and PHR concerning group dynamics (Section 5). [4]
Empowerment is a crucial concept in PHR and is informed by an emancipatory paradigm (BORDA, 2006 [2001]). FREIRE (1970,1968) is often referred to in literature with this concept. The concept of empowerment has been widely discussed (BLACKBURN, 2000; CASTRO, VAN REGENMORTEL, VANHAECHT, SERMEUS & VAN HECKE, 2016; RAPPAPORT & SEIDMAN, 2000; VAN REGENMORTEL, 2002; ZIMMERMAN, 2000), but a universal definition is yet to be produced. Empowerment can be identified as an essential promoter of health, while the role of powerlessness is seen as a risk factor for disease. Empowerment is therefore seen as a health-enhancing strategy (WALLERSTEIN, 1992) or as a way to develop an "empowering society" (VAN REGENMORTEL, 2002, p.75). An empowering society is a society that responds creatively to the capacities of individuals, organizations, groups, and communities, leaving room for autonomy, stimulating partnerships, and providing reinforcement where necessary. In a society like this, there is attention to structural mechanisms of social exclusion, and opportunities for everyone are promoted through active participation. [5]
FREIRE (1970 [1968], p.493) relates empowerment to "conscientisation" and "critical consciousness." Conscientisation refers to the process in which persons become more aware of the sources of their oppression. FREIRE sees conscientisation as the first step in achieving empowerment. It is a process in which the capacity for critical thinking is enhanced. He refers to four levels of critical consciousness of socio-economic-political positioning: the magical, the naïve, the critical, and the political level. The political consciousness is the level at which people discover that others share their perception of reality and experienced problems. FREIRE's work implies that empowerment is a process of developing strength vis-à-vis one's environment, i.e.:
"We can legitimately say that in the process of oppression someone oppresses someone else; we cannot say that in the process of revolution someone liberates someone else, nor yet that someone liberates himself, but rather that human beings in communion liberate each other" (p.66). [6]
Scholars see empowerment as a process and an outcome that applies to individuals, groups, organizations, and entire communities (PRILLELTENSKY, 2008; VAN REGENMORTEL, 2002; ZIMMERMAN, 2000). PRILLELTENSKY (2008) describes the interrelatedness of power, well-being, oppression, and their influence at personal, relational, and political levels. On a personal level, this includes gaining a locus of control, critical awareness, and developing skills and competencies. Empowerment is fostered and sustained by relational and social support, which can lead to the development of a sense of belonging and collective action in a group. Empowerment also has a political component, which includes the mobilization of political and economic power to strive for social justice. In sum, empowerment is an open-ended, multi-level, dynamic, and multi-faceted concept that can help to make sense of the value of participatory processes for greater social justice and change. [7]
In 2015, a charity organization in the Netherlands initiated a 5-year program (2015-2020) to promote the well-being of families who live in areas of social disadvantage. The level of involvement of the people who were to benefit from the program varied in 46 sponsored projects. In 2016, the officer of the charity organization signaled a need for higher level of participation of the people they wanted to support in the sponsored projects as well as in their organization. At that moment, family members did not have a voice in the call for proposals in 2015, did not participate in the ongoing evaluation or monitoring of the sponsored projects, and did not have a seat on the charity board of the program. The charity fund wanted to sponsor an "open project" to stimulate participation in the current and upcoming programs of the charity fund and approached us (authors) to facilitate such a participatory project. [8]
The project started with one mother, who lived in circumstances that the program of the charity fund wanted to challenge, and the first author (Barbara) who approached the mother as co-initiator. The mother and a colleague of Barbara had already worked for two years together on another research project. Working from the start of a PHR study together with people who live or work in the subject of the project is an important principle of PHR (ABMA et al., 2019; ICPHR, 2013a). In informal ways, Barbara got in touch with four other mothers. They all reacted to a flyer with the heading: "Did you have a hard time at home, but do you feel better now? Share your experiences with the charity fund." The promise to the mothers was that they could formulate their own (research) aims, questions, and jointly design the project. The women received financial compensation for their time and travel expenses per meeting. [9]
The five mothers all live in a situation of poverty. Three of them are single mothers, and one got divorced during the period of the action group. They all experience different impairments. The age of the children varied (the youngest was 3, and the oldest 18 years) as well as their ethnicity and country of birth of the mothers. Some went back to school recently to increase their job opportunities, and some did voluntary jobs in their neighborhood. From now on, the group of women, facilitated by Barbara, will be called "the co-research group." The co-researchers who live in poverty are named "the mothers." [10]
We (Barbara and Tineke) are both affiliated with a university. Barbara is a researcher, Ph.D. student, and teacher, who has conducted PHR for five years. Tineke is her Ph.D. supervisor, a professor in the field of participation and diversity and acted as a critical friend in the study and co-author. We share many privileges as we are both white, heterosexual, married mothers from middle-class backgrounds who are well educated, able-bodied, and employed. At the same time, we shared the challenges, difficulties and rewards of engaging in a PHR project over five years with different groups of people in unfortunate situations in academic and community environments. Both of those are sometimes hostile towards this type of research. In addition, two officers of the charity organization, a creative artist and a research-journalist, were connected with the co-research group to bring ideas and resources when necessary. The officers of the charity organization were more deeply involved in the group. The others were involved at moments in which the group thought they could use support, including competences, knowledge, and network. [11]
We named the PHR study You Do Not See It after a booklet designed by the mothers in this study. We chose this name, because "not being seen" and "judged by labels and prejudices" appeared as central themes in the lives of the mothers. [12]
3.3 Participatory health research
The goal of PHR is to maximize the participation of people whose life or work is affected by the study and who can contribute to the study given their experiences. This participation covers all phases of the study (ICPHR, 2013a). The co-research group started the project by creating its agenda for research and action. Although the program of the charity fund focused on changing behavior related to unhealthy lifestyles, like food, smoking, sports, exercise, and alcohol use, the group decided not to focus on healthy lifestyles. The members acknowledged that an unhealthy lifestyle does not promote health and well-being; however, they believed that other topics were more critical in their lives. In their opinion, the mothers' unhealthy behavior was an outcome of underlying problems, like stress, low income, being a single mother, loneliness, mental issues, not feeling worthy, and having no job. All of these issues related to oppression (PRILLELTENSKY, 2008). So they felt the root causes needed to be addressed instead of working on behavioral changes. [13]
The co-research group conducted three research projects in two years together with the collaborators. In this article, we highlight two research projects. The focus of the first project was increasing participation of families in funded projects. The central question was: how can professionals of funded projects (project leaders, professionals in health and well-being, care workers, and researchers) collaborate with mothers in funded projects? In their second project, they aimed to promote action on a national level. Their second research question was: what are barriers to well-being for mothers in stressful situations? (Table 1) [14]
3.4 Ways to collaborate with the mothers
As a research group, we decided to make an appointment once every two weeks on Monday mornings on school days. From the first moment, the mothers strongly articulated their wishes and demands in collaboration. As a group, we decided on several criteria for our collaborative work. We agreed to 1. be meaningful, 2. help others with our experiential knowledge, 3. act (not just talk), 4. create something that made us proud, and 5. reach people "with power" on a local and national level with our products and voices. We wanted to learn by doing and wanted to evaluate our collaboration in a participatory way at several moments in the process. [15]
The research group meetings with the mothers were central to the whole PHR process. We used the following participatory methods: single and joint interviews, group meetings, reflection questionnaires, photo-elicitation, and other creative methods (Table 1). The study is still ongoing at the moment of writing. Therefore, we shall describe the time period 2016-2018.
Table 1: Overview of the PHR project You Do Not See It (2016-2018). Please click here to download the PDF file. [16]
Our reflection of the use of participatory methods and the interactions among the mothers participating in the study is based on additional qualitative data sources (Table 2). These sources are transcripts of the meetings and evaluations of the meetings with the co-research group, field notes, and diary notes of Barbara. Together, we analyzed all data sources, with the research question in mind, and empowerment and critical consciousness as sensitizing concepts.
Table 2: Overview of reflection material. Please click here to download the PDF file. [17]
The mothers granted their consent to participate in this research project. According to the ethical principles of the ICPHR (2013b), we started the project with conversations about the questions: Why do we want to work together? and What are the aims of the projects? We also discussed power, ethics, and responsibilities and the main principles of ethical PHR (BANKS & BRYDON-MILLER, 2018; ICPHR, 2013b) in the first few sessions. The mothers appeared to be motivated to spend time on the dissemination of their findings to a Dutch audience. They did not collaborate in writing the present academic text. [18]
For privacy, we used pseudonyms and shuffled names with quotes. All quotes were member-checked during the process with the individual members. Just before submitting this article, we translated the quotes by a native speaker to prevent any loss of meaning during translation (VAN NES, ABMA, JONSSON & DEEG, 2010). [19]
In this section, we describe the non-linear, dynamic, and iterative process of collaboration of the co-research group in the PHR study You Do Not See It. We have outlined the participatory process, followed by a reflection on the process to foster empowerment. [20]
4.1 Personal understanding through storytelling
In 2016, we got to know each other—the mothers, the officers of the charity fund, and Barbara. We shared stories about our lives and photos of our family and living environment. Besides, we discussed media portrayal of "people living in deprived neighborhoods" to get to know each other. We examined what it meant to live in poverty by sharing stories. It became clear that three of the five mothers were pretty critical of the structural forces that led to their poverty.
Nicky: "Society demands high standards but is not set up to support people like my son. If your legs stop working, you get a wheelchair. But my son does not receive adequate support. Society wants you to participate, have power for that, etc., but you don't receive any tools that help you to participate."
Anouk: "That gap is simply increased by what is going on in the whole world. Life moves so quickly, and everything is digital these days, and in such a rapid tempo. And the money is in the hands of certain groups, and they determine for the system how it will work in the entire world. Companies and the government do not want to see the best of us as people. They only look to see if we add a profit." [21]
These rather critical mothers all went back to school for a degree in experiential knowledge of intergenerational poverty and social exclusion before or during the project. They became critical of structural inequalities in society through this training. Two other women were less critical and lived more by the day. One mother felt that she was a victim of the situation and partly attributed this to herself.
Zahra: "My life is a struggle. Always has been, and it will probably always stay that way. Maybe it's my destiny. Could be ... at some point, you get confused or do not know how to solve everything. Then, I negatively express myself. You should but cannot find a way to keep going. I have always found it difficult to ask for help because I have too much pride, but I also feel a kind of sadness!" [22]
After three meetings, the mothers concluded that projects which focused only on a healthy lifestyle did not best meet the needs of the families that should benefit from the projects. They wanted to contribute to the root causes of unhealthy behavior.
Anouk: "Many people talk about 'everyone has to live a healthy life, no smoking or drinking, you name it.' But why are there these situations? Why does this happen to people? People start to smoke and drink out of despair, and that has nothing to do with disabilities. Their lives are limited because they have less income and do not know how to keep going. Smoking is not the first problem to solve." [23]
In the beginning, the atmosphere in the group was warm. The relationship between the mothers showed tenderness. When co-researchers told stories about experiences of difficulties in daily life, other co-researchers reacted sensitively and empathically. They seemed to understand the position of the other, as they knew by experience how it felt and often gave advice about how they should deal with the situation. In the meetings and a WhatsApp group of the co-research group, the women supported each other during hard times. However, occasionally, we all were aware that the atmosphere became slightly tense. Most women wanted to be heard, but in practice, they did not precisely listen to each other. Two women explicitly criticized the opinions of each other all the time. Barbara wrote in her diary: "It is not yet a group. The mothers respond to each other only if they recognize themselves in the story of the other. Mostly, they do not examine each other's experience." [24]
Reflection on the process
In this first phase, the women got to know each other, the co-researchers of the charity fund, and Barbara. Articulating each other's lens of understanding is part of PHR because this provides understanding of each other's frame: what we see and how we define situations, problems, and solutions (ABMA et al., 2019). The group defined health broadly and wanted to focus on root causes instead of individual lifestyles. This can be considered the first step towards critical consciousness; instead of a narrow biomedical framework, the women framed it in a broad, holistic way (HUBER et al., 2011). Moreover, in a short period, they set their agenda for the research project and actions for change. The group found common ground and developed its agenda that deviated from the original focus of the charity organization. This was an important political statement: the mothers did not follow the agenda of the most powerful party but created their own agenda based on their own experiences and framework. [25]
While we experienced tensions in the group, our first reaction was to reflect on it with colleagues from a third-person perspective (REASON & TORBERT, 2001). A colleague encouraged Barbara to reflect on her personal position as a facilitator in the group. This was uncomfortable. Barbara, as a facilitator, was aware of her otherness; she lived in a different situation, having had different educational opportunities, had a job and experienced the impairment that she could not understand the situation of the women fully. Nevertheless, Barbara was not fully aware of her role in the tensions. For the mothers, she was the facilitator who set the standards. We decided to discuss some moral principles of PHR in-depth, like mutual respect, equality, and inclusion in the group. We also wanted to share the responsibility for the atmosphere in the group with the members. [26]
4.2 Mutual understanding through interactions with stakeholders
In the second phase, the group started with its first project about participation. As said before, the charity fund emphasized the importance of the participation of family members in the projects to ensure success and continuation. In practice, however, professionals of the funded projects often experienced difficulties in collaborating with fathers, mothers, and children in challenging circumstances. [27]
To explore this phenomenon, the mothers first briefly shared their first-person experiences about participation in projects in their neighborhood.
Zahra: "People who are poor, like me, find the atmosphere of a project important. It should be fun. Sociability is scarce in our life. I saw that some professionals acted like: yes, this is my day, and this is my time, I do not have that much time, I have to do this and that. That mentality! So especially that informal, looser, not too tight, I like that."
Nicky: "The people of the health service and the hospital always have such a negative attitude towards me when they talk about health. They reject my behavior. During these moments, I immediately think: 'Am I doing something wrong? Is my childcare not good enough?'" [28]
The co-research group invited professionals of funded projects to share their experiences of difficulties in collaborations with family members by a survey with open questions. The co-research group drafted a series of questions for the survey. In the next group meeting, we discussed the findings from the survey forms (n=20). Each participant of the survey received a personal reaction from the mothers, with an invitation to join a co-researcher group meeting for a face-to-face encounter. [29]
Sixteen professionals from 12 funded projects met the group in face-to-face group meetings. These meetings resulted in a vast knowledge base about the complications which the professionals experienced with the involvement of families and the reflections of the mothers on these difficulties. The mothers liked face-to-face encounters; it fit their ideas on collaboration. They helped professionals of funded projects by sharing experiential knowledge. Initially, the mothers were uncertain about their contribution, but when professionals confirmed that the experiential knowledge was complementary to their own practical and scientific knowledge, they became convinced that their contribution was respected. [30]
After the meetings with professionals, we discussed that designing a brochure with all our insights and experiential knowledge would be a good way to disseminate the findings of this project. However, while doing this, a mother raised a question, which showed her insecurity and needs for acknowledgment: "We think that it is valuable to share our knowledge in a brochure, but how did the project leaders experience the meetings and how did they use our insights in practice?" (Janis) [31]
We decided to e-mail all professionals we had met for their reflections on the encounter. With a 100% response rate and substantive feedback, we concluded that many had integrated pieces of the mothers' advice into their project; some even said that the appointment had a significant influence on the way they worked. Only a few did not do anything (yet) with the insights of our encounter. We saw these positive results as a confirmation again that the voice of the mothers was heard, and that the knowledge had value for the professionals.
A project leader: "We decided to do things differently after our meeting. And perhaps less concrete, but also important, we have been organizing more involvement and input from residents during the last few months, for example in health prevention interventions, evaluations from questionnaires, etc. Very desirable and this also improves the quality of service." [32]
Mothers were also proud of the brochure (Figure 1) they made: "I love this summary. It answers the question of how to collaborate with families in funded projects from our perspective. It brings all our conversations together in a few pages" (Zahra).

Figure 1: The cover of the brochure about participation for professionals [33]
Looking at the group dynamics in this phase, we saw a mixed picture. At some moments the ambiance was pleasant, especially when the professionals visited the group. However, there were still tensions in the group. For example, mothers were explicitly looking away when a mother spoke not-so-fluent Dutch or if someone talked for too long or too much about her misery and pain. Some mothers also gave non-verbal signals as rolling eyes and raising a cold shoulder at these moments. Having a full and inclusive dialogue was not always easy. Some mothers shared with Barbara that they recognized the atmosphere in this group is similar to the atmosphere in other groups they joined. They shared with Barbara in a one-on-one conversation their understanding of the atmosphere:
Joyce: "The group is a fight. Jealousy. Who simply takes control of the group? The group is so vulnerable. Everyone can be hurt so quickly."
Janis: "Your life is so small; your life is your home and your television. You do not experience a whole lot, so you just want to say: I also know something, I also want to be a part of things, I am there too, I am also somebody and I want to contribute something. Those kinds of feelings are very present at these meetings." [34]
Reflection on the process
The mothers shared their stories in dialogue with professionals of funded projects. They were heard and felt acknowledged. The women experienced in most meetings that they were valuable speakers and did not experience negative judgments of their identity from professionals of funded projects. This experience differed from their usual experiences where they felt judged on stereotypes of women in poverty and were not taken seriously as a credible knowledge sharer. [35]
The mothers' horizon broadened. The encounters with new people were pleasant. Living in poverty meant for some mothers that they did not leave their home or neighborhood often; their world had become small. We created opportunities to meet and connect with people and to learn about projects all over the country through these participatory actions. The group gained access to new knowledge and experiences and people they otherwise never would have met. They also felt valuable by sharing their knowledge. It created a sense of ownership and pride and a sense of belonging to a community that helped create a better world for their peers. [36]
By the start of the PHR study, we had already met as a group 14 times. We observed that polarization around interpersonal issues continued between some mothers. It seemed that the mothers normalized the conflicts and got familiar with this kind of interaction in the group. One intervention of Barbara, as a facilitator, was one-to-one conversations about the atmosphere in the group (second-person reflection). This gave us some insights into the understanding of the group members on the group dynamics, and she could ask for their cooperation for a good atmosphere during the meetings. Despite these conversations, we did not break through the battle for power between the group members. However, as a facilitator, she could feel more connected to the members due to the mutual understanding. [37]
4.3 Deepening personal understanding: More creative methods
Inspired by the success of the brochure, we decided as a group to prepare a booklet. Most mothers wanted to show the world the impact of living in an unfortunate situation on their family and their health situation. We started with two brainstorm meetings to talk about the booklet and decided that the booklet should be an invitation to policymakers to understand the world of the mothers and families and to reframe the poverty problem from the perspective of mothers. The women found two topics crucial: stories about the emotion of "gekwetste binnenkant" [being hurt inside] (SPIESSCHAERT, 2005, p.39; SUIJS, 2012) and experiences of friction between lifeworld and system (HABERMAS, 1987 [1981]). [38]
At first, we collaboratively explored the concept of feeling hurt inside. We organized in-depth joint interviews with the women; the women themselves conducted and audiotaped the interviews. We did a member-check by the women of the transcripts in the next meeting. We shared the narratives of the women from the transcripts in anonymous quotes with the group on the wall. This stimulated discussion about the quotes. At the meeting, one woman started to share (funny) quotes that circulated online in the WhatsApp group of the co-research group, because the quotes on the wall stimulated her. That evening, the mothers shared over 100 quotes on the WhatsApp group. For most mothers, these quotes were a way to communicate with loved ones and to express their feelings when they did not have the words for it.
Anouk: "Sorry, this is my way of communication" [when she posted 50 quotes in 10 minutes].
Janis: "Yeah, this is fun." [39]
In the next sessions, the mothers discussed the WhatsApp quotes and which ones people related to, or not, and why (Figure 2).

Figure 2: Discussing quotes and photos with the co-research group [40]
Then, a creative artist joined the group sessions. She brought in a fresh idea of using photography in the process to capture the essence of what it means to be a mother dealing with poverty and the challenges related to their situation in visuals and stories. The group welcomed a new and creative person. The creative artist renewed the discussion because she used alternative ways of exchanging perspectives about poverty and the feeling of "being hurt inside" with an art-based approach. After a short camera training in the session, the mothers were asked to take pictures of their lives with their mobile phone in the following two weeks. The mothers sent their photos to the creative artist who printed them for the next meeting. In the meeting, we discussed the pictures with each other, using the first three questions of the SHOWeD-method (WANG & BURRIS, 1994; WANG, YI, TAO & CAROVANO, 1998) to explore the stories behind every image. Every photograph brought us to stories that were not obvious upon first seeing the picture. At that moment, the central theme You Don't See It emerged. [41]
Through the use of photography, themes that were difficult or painful to talk about were discussed, and this deepened the understanding of "hurt inside" and You Don't See It. We discussed themes as vulnerability of a child from a low-income family in society, the responsibility of the mothers to their children, and loneliness and stigmas facing the mothers. Some mothers were helped to alleviate their misery by exchanging these themes: "I am impressed by the stories of others who have a harder life than I do" (Joyce). [42]
Another theme that stood out in all the narratives of the mothers were negative experiences with "the system" (governments and other institutions they depend on). We noted that every person had a different story, and every story needed to be heard and seen by others. An external research-journalist conducted interviews with the mothers and wrote a short story for each person. From that moment on, we started a conversation to explore together why these negative experiences existed within the system. For some mothers, it seemed like a simple question; for others, it was a very complicated question.
Nicky: "We are all stuck within the system."
Anouk: "It is from both sides, how can we [policymakers, professionals, and mothers like me] listen carefully to each other? Without blaming anyone? That is complex."
Janis: "... I do not know ..." [silence]
Zahra: "Nowadays, companies and policymakers only look at the question: what is this person going to perform? So they only hire temporary people, only investing in the 'high potentials.' It is a grey area. You need to perform at a very high level to participate in society. If you do not fit into their picture, you have bad luck and belong nowhere. Then you sit at home, nobody will help you, and they say: it is your fault. But they do not see that people have other qualities. They are too focused on ..."
Joyce: "... yes ..." [silence] [43]
After the conversation about the background of the current unjust situation, we had a dialogue about what needs to change for social justice. A lot of insight emerged by doing a creative assignment with the aim to have a dialogue about this topic. In the assignment, we looked from different perspectives (the person, helpers, organizations, and laws) to see solutions. The mothers saw that from all sides, including policymakers and politicians, professionals and mothers, joint actions were necessary to change.
Nicky on the ideal situation of acknowledgment of experiential knowledge by policymakers: "Well, I notice that in my municipality: collaboration works ... If you can reach the same conclusion together, you can really get somewhere. I notice that this works."
Anouk on professionals who annoy her: "I am not retarded. You think in boxes and labels. That's how it works. So try to let go of all those stereotypes and see me as a human being."
Janis on the role of mothers and their attitude: "At a certain moment, we do not see them [professionals] as people either. I notice it in myself. Recently, I reflected on my behavior: I was just rude to her [professional]. What did she do to me? It is just her job. So I also have to change." [44]
The creative artist designed the booklet of the co-research group, with figures of silver ink on every page. The visuals would remind us of a broken coffee cup that was fixed (Figure 3), as a reference to "hurt inside." You do not see the hurt inside because it is "fixed" from the outside, and we, as mothers, make it beautiful. But if you look closely, then you understand the hurt inside and its impact. The booklet is in the process of printing. A meeting with the co-research group and the Minister of Health is on the agenda.
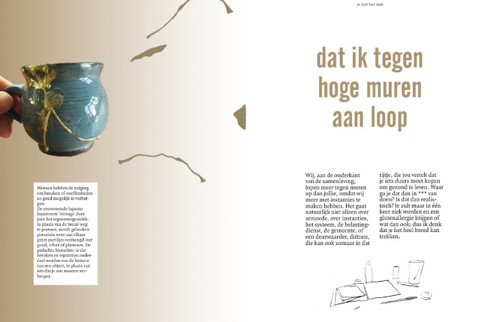
Figure 3: One of the pages of the booklet about the broken cup [45]
The atmosphere changed positively in the group by working with a creative artist. We were more focused on the project than on each other by different assignments to collaborate on and different questions that were asked. Besides, the "do"-element of working with photographs and finding quotes helped to give the mothers a sense of ownership over the booklet. The material is theirs, and the professionals assisted in analysis and writing. [46]
However, we still saw that the frictions in the group continued. The co-researchers reflected on this situation:
Janis: "All those years, you are stuck in that painful situation...You cannot imagine how miserable those situations are. Sometimes, horrible things happen. I keep it to myself. I have lived through a war for eight years. You cannot imagine how horrible it can be. And that kind of revolution, the regime has changed, and the oppression, all of that, that I escaped my own country. Then you go to another country without speaking a word. You just have to, and I am so tired of it. I have absolutely no millimeter room for all those people who speak about their poverty [in this country without war]."
Nicky: "I just don't have room and patience for other people right now, because I am so stressed, hurt and broken." [47]
Reflection on the process
In this third phase, the mothers developed a booklet about Hurt Inside and the barriers they face as a mother living in poverty. We made fun of the negative prejudicial stereotypes facing mothers in poverty. Humor and creativity were essential coping mechanisms in the process. Being ironic helped to reflect on themselves. The process of reflection stimulated a positive vibe in the group. "Having fun" was helpful in the occasionally tense process. [48]
We used a series of creative methods. By using art-based techniques (GERGEN & JONES, 2008), it appeared to be less challenging to share stories of painful themes that had appeared to be hard to articulate before. Some mothers found strength in this way because they learned that they were not the only ones who experienced the impact of poverty. Besides, sharing personal stories and the photographs of their lifeworld in a booklet to the outer world could be seen as a facilitator for political empowerment. [49]
The collaboration with the artist and art-based methods helped deepen the group's understanding and develop artifacts that helped them to reach out to the "others," namely policymakers, professionals in care and prevention, and the people from the charity fund. Their story was presented in a tangible product and contained very personal qualitative and creative material that easily touched others. The mothers valued these artifacts as conversation pieces with officers of the charity fund in this case, who listened very carefully and were open to their accounts. [50]
Within the group, we saw group dynamics that enhanced and decreased empowerment. On the one hand, we saw that the mothers, who already had developed critical consciousness before the start of the project, were the drivers of the political engagement in the co-research group. They stimulated others to reflect critically and reach out to "others." On the other hand, we saw that the group dynamics also influenced the vibe in the group negatively. FREIRE (1970 [1968]) states that people who experienced oppression in their past in whatever situation are often shaped by that experience. They are hurt inside, exactly as we described in the booklet. Being hurt and oppressed is painful, generates anger, and leaves scars. Trusting people was not easy. This influenced the way we connected. A few times, we tried to discuss this in the group, but it was difficult to have an open discussion and reflect on it in the group to make a change. [51]
In this study, we learned about pathways and challenges to working in PHR to foster personal, relational, and political empowerment. On a personal level, empowerment seemed to have taken place by a variety of paths in this PHR study. First of all, sharing control over the agenda of the research project, and the way we worked were essential steps for the mothers. Shared ownership is a core principle of PHR (ABMA et al., 2019; ICPHR, 2013a) and an empowering society (VAN REGENMORTEL & FRET, 2000, p.302). Along the way, the mothers felt more and more responsible for the process and outcome of the research projects, and proud of the products. Secondly, acknowledgment of the professionals provided by feedback-loops in this study seemed to provide a positive influence on the mothers' self-assurance and self-consciousness. In their lives, the mothers often experienced epistemic injustice (FRICKER, 2007) by professionals—being seen as incredible knowers because of negative identity-prejudicial stereotypes (CRICHTON, CAREL & KIDD, 2017). In this PHR context, however, epistemic justice was experienced. Thirdly, we fostered learning and broadened horizons of people involved in the study. In this PHR study, we learned via co-creation about collaboration, living in poverty, and underlying structures. Our learning influenced our level of critical consciousness (FREIRE, 1970 [1968]). Fourthly, using humor to critically reflect on, and look with, irony to oneself was important in this process (MUNN-GIDDINGS & COOK, 2016). Finally, by participating in this PHR study, the mothers met people with stories, gained knowledge, and built networks. It enlarged their world and moved them away from their living room at home. This form of access to knowledge and networks (WANG & BURRIS, 1994) fostered individual empowerment. We also see in this process the value of volunteering for health and well-being (COHEN, 2009). [52]
In our study, we mostly learned about the challenges of relational empowerment. The relational dynamic between the women was occasionally tense; polarization around interpersonal issues and in-group-conflicts were normalized. In this study, we reflected on three different levels (REASON & TORBERT, 2001) to understand the specific relational situation. We reflected via individual self-inquiry (first-person), with people from the co-research team (second-person) and with others from a broader community, like PAR colleagues and the literature (third-person). From second-person reflections, we learned that tensions were rooted in deeper emotional states of the people contributing to this study. In third-person reflections, we used the literature on poverty and oppression to understand the situation. [53]
In our reflections, we firstly related the interactions in the group to the concept of an "empathy wall" (HOCHSCHILD, 2016, p.5). Tensions mostly occurred between a mother with a refugee background and two women born and raised in the Netherlands. An empathy wall is "an obstacle to the deep understanding of another person, one that can make us feel indifferent or even hostile to those who hold different beliefs or whose childhood is rooted in different circumstances" (ibid.). Being raised in poverty in a country with war and oppression is different from being raised in poverty in a Western-European country. Secondly, the concept of hurt inside describes a deep emotional sadness that hindered people in poverty from functioning due to feelings of inferiority, confusion, being misunderstood, not accepted, shame, guilt, and humiliation (SPIESSCHAERT, 2005; SUIJS, 2012). This feeling of hurt inside could influence every contact with others. Finally, the concept of "horizontal violence" (FREIRE, 1970 [1968], p.62) helped us to understand group interactions. Manifestations of "horizontal violence" in a group include, besides more aggressive ones, subtle nonverbal behavior such as rolling eyes and raising a cold shoulder (THOMAS, 2012). The concept "horizontal violence" is characteristic for oppressed groups that fight others at the same level of a hierarchical system because they cannot be angry at people with power (ROBERTS, 1983). [54]
The concepts described above helped us to better understand the group dynamics, and how the interactions in the group worked. The drivers for the tensions in the group seem to be rooted in the lives of the mothers. Understanding their responses increased our compassion and empathy with the women and helped us to relate with all of them respectfully. It also helped us to stimulate mutual understanding among the mothers. [55]
The focus and attention to the group dynamics distracted us from focusing on the discussion of structural causes of exclusion. The relational dynamics required "ethics work" (BANKS, 2016, p.35) for Barbara: putting effort into seeing ethically salient aspects of situations and developing oneself as a good facilitator who stimulated the empathy and mutual understanding within the group. Therefore, we only slightly fostered political empowerment and mobilization of resources in this PHR study. We saw that in this study, structural factors of poverty, like having no paid jobs, low education, and low health status, were internalized and individualized by some of the women. Discussing these topics was painful and made some people silent and sad. Remarkably, we saw the power of education on experiential knowledge and the development of levels of critical consciousness. The mothers who were trained to use their experiential knowledge were much more aware of their position and sources of oppression and inspired the others who did not have the educational input. Although it fostered everyone's capacity for critical thinking to some extent, it was only a first minor step to political empowerment of the group. Discussion of structural sources of exclusion requires attention and time before a group comes to collective action on a political level. [56]
Finally, we highlight with this study that participatory methods promote empowerment, especially with the use of a creative, performative and arts-based approaches in data generation and knowledge translation (BOYDELL, GLADSTONE, VOLPE, ALLEMANG & STASIULIS, 2012; GERGEN & JONES, 2008; MITCHELL, DE LANGE & MOLETSANE, 2017; NGUYEN, 2018; VAN DER VAART, VAN HOVEN & HUIGEN, 2018; GUINEY YALLOP, LOPEZ DE VALLEJO, & WRIGHT, 2008). Creative assignments and arts-based methods supported participation (WOODGATE, ZURBA & TENNENT, 2017) and brought deep and informed understanding of complex issues (ABMA et al., 2019). In this case, the use of creative methods helped to express shameful and painful experiences that were hard to express by words alone. Moreover, the use of performative language, aesthetic writing, photography, and metaphors could create conduits for emotional connections and the delivery of messages that are deeply embodied and difficult to express (WOODGATE et al., 2017). They could be used as invitations to others to "consider this way of seeing the world" (GERGEN & GERGEN, 2010, §2). Arts-based approaches could cross boundaries and connect with others as a "boundary object" (WOODGATE et al., 2017), which could be a step in reaching out and political empowerment. [57]
The strength of this study is the detailed description of a PHR process, in which the reader could learn from an example of PHR. Besides, we give insights into the precarious process of PHR and group dynamics and show the vulnerability of the mothers and facilitators in a process of co-creation. The most important limitations of the study are that the concept of empowerment is not adequately elaborated on together with the mothers. We present in this article the perspective of the authors, based on data collected at various moments. However, it could be that the mothers have a different perspective on the topic of empowerment, what this PHR study has brought them, and what has held them back from empowerment. [58]
The first years of this PHR study with mothers living in poverty contributed to empowerment on several levels. Mainly, personal empowerment was achieved by different means, mainly by the promotion of ownership and epistemic justice. In this case, achieving relational and political empowerment was more challenging. Relational dynamics influenced the process, and focus of the group and facilitator, and the relational-ethical work distracted us from gaining political empowerment. We conclude that time, relational sensitivity, and perseverance are essential to achieving empowerment on all levels in PHR. Navigating in a PHR journey between personal, relational, and political elements of empowerment is complex but full of potential benefits for all parties involved. [59]
We gratefully acknowledge the support the all those involved in the PHR study, including Marielle SCHUURMAN as scholarly artist.
Aamann, Iben Charlotte (2017). "Oh! Iben's here now, so we better behave properly"—The production of class as morality in research encounters. Forum Qualitative Sozialforschung / Forum: Qualitative Social Research, 18(3), Art. 7, http://dx.doi.org/10.17169/fqs-18.3.2752 [Accessed: October 6, 2019].
Abma, Tineke; Banks, Sarah; Cook, Tina; Dias, Sónia; Madsen, Wendy; Springett, Jane & Wright, Michael (2019). Participatory research for health and social well-being. Cham: Springer.
Adili, Fatemeh; Higgins, Isabel & Koch, Tina (2013). Older women and chronic illness: Transitioning and learning to live with diabetes. Action Research, 11(2), 142-156. https://doi.org/10.1177/1476750313477157 [Accessed: October 6, 2019].
Banks, Sarah (2016). Everyday ethics in professional life: Social work as ethics work. Ethics and Social Welfare, 10(1), 35-52, http://dro.dur.ac.uk/18036/1/18036.pdf?DDD34+dss0sjb+dul4eg [Accessed: October 6, 2019].
Banks, Sarah & Brydon-Miller, Mary (Eds.) (2018). Ethics in participatory research for health and social well-being: Cases and commentaries. Abingdon: Routledge.
Blackburn, James (2000). Understanding Paulo Freire: Reflections on the origins, concepts, and possible pitfalls of his educational approach. Community Development Journal, 35(1), 3-15.
Borda, Orolando Fals (2006 [2001]). Participatory (action) research in social theory: Origins and challenges. In Peter Reason & Hilary Bradbury (Eds.), Handbook of action research: Participative inquiry and practice (pp.27-37). London: Sage.
Boydell, Katherine; Gladstone, Brenda; Volpe, Tiziana; Allemang, Brooke & Stasiulis, Elaine (2012). The production and dissemination of knowledge: A scoping review of arts-based health research. Forum Qualitative Sozialforschung / Forum: Qualitative Social Research, 13(1), Art. 32, http://dx.doi.org/10.17169/fqs-13.1.1711 [Accessed: October 6, 2019].
Castro, Eva Marie; Van Regenmortel, Tine; Vanhaecht, Kris; Sermeus, Walter & Van Hecke, Ann (2016). Patient empowerment, patient participation and patient-centeredness in hospital care: A concept analysis based on a literature review. Patient Education and Counseling, 99(12), 1923-1939.
Cohen, Ayala (2009). Welfare clients' volunteering as a means of empowerment. Nonprofit and Voluntary Sector Quarterly, 38(3), 522-534.
Cook, Tina; Boote, Jonathan; Buckley, Nicola; Vougioukalou, Sofia & Wright, Michael (2017). Accessing participatory research impact and legacy: Developing the evidence base for participatory approaches in health research. Educational Action Research, 25(4), 473-488.
Crichton, Paul; Carel, Havi & Kidd, Ian James (2017). Epistemic injustice in psychiatry. BJPsych Bulletin, 41(2), 65-70, https://doi.org/10.1192/pb.bp.115.050682 [Accessed: October 6, 2019].
Freire, Paulo (1970 [1968]). Pedagogy of the oppressed. New York, NY: Bloomsbury.
Fricker, Miranda (2007). Epistemic injustice: Power and the ethics of knowing. Oxford: Oxford University Press.
Gergen, Mary & Gergen, Kenneth J. (2010). Performative social science and psychology. Forum Qualitative Sozialforschung / Forum: Qualitative Social Research, 12(1), Art. 11, http://dx.doi.org/10.17169/fqs-12.1.1595 [Accessed: November 15, 2019]
Gergen, Mary & Jones, Kip (2008). Editorial: A conversation about performative social science. Forum Qualitative Sozialforschung / Forum: Qualitative Social Research, 9(2), Art. 43, http://dx.doi.org/10.17169/fqs-9.2.376 [Accessed: October 6, 2019].
Habermas, Jürgen (1987 [1981]). The theory of communication, Vol. 2: Lifeworld and system: A critique of functionalist reason. Oxford: Polity Press.
Hochschild, Arlie Russell (2016). Strangers in their own land: Anger and mourning on the American right. New York, NY: The New Press.
Huber, Machteld; Knottnerus, J. Andre; Green, Lawrence; van der Horst, Henriette; Jadad, Alejandro; Kromhout, Daan; Leonard, Brian; Lorig, Kate; Loureiro, Maria Isabel; van der Meer, Jos; Schnabel, Paul, Smith, Richard; Weel, Chris van & Smid, Henk (2011). How should we define health?. British Medical Journal, 343, d4163.
ICPHR (International Collaboration for Participatory Health Research) (2013a). Position Paper 1: What is participatory health research?. Berlin: International Collaboration for Participatory Health Research, http://www.icphr.org/uploads/2/0/3/9/20399575/ichpr_position_paper_1_defintion_-_version_may_2013.pdf [Accessed: October 6, 2019].
ICPHR (International Collaboration for Participatory Health Research) (2013b). Position Paper 2: Participatory health research: A guide to ethical principles and practice. Berlin: International Collaboration for Participatory Health Research, http://www.icphr.org/uploads/2/0/3/9/20399575/ichpr_position_paper_2_ethics_-_version_october_2013.pdf [Accessed: October 6, 2019].
Mitchell, Claudia; De Lange, Nadene & Moletsane, Relebohile (2017). Participatory visual methodologies: Social change, community and policy. London: Sage.
Munn-Giddings, Carol & Cook, Tina (2016). Editorial. Concluding thoughts: Virtual issue on the theme of "creative expression" in action research. Educational Action Research, https://www.tandf.co.uk//journals/pdf/EARJ-VSI-Editorial.pdf [Accessed: October 6, 2019].
Nguyen, Megan (2018). The creative and rigorous use of art in health care research. Forum Qualitative Sozialforschung / Forum: Qualitative Social Research, 19(2), Art. 21, http://dx.doi.org/10.17169/fqs-19.2.2844 [Accessed: October 6, 2019].
Pillow, Wanda (2003). Confession, catharsis, or cure? Rethinking the uses of reflexivity as methodological power in qualitative research. International Journal of Qualitative Studies in Education, 16(2), 175-196.
Prilleltensky, Isaac (2008). The role of power in wellness, oppression, and liberation: The promise of psychopolitical validity. Journal of Community Psychology, 36(2), 116-136.
Rappaport, Julian & Seidman, Edward (Eds.) (2000). Handbook of community psychology. Berlin: Springer.
Reason, Peter & Torbert, Wilbert (2001). The action turn: Toward a transformational social science. Concepts and Transformation, 6(1), 1-37.
Roberts, Susan Jo (1983). Oppressed group behavior: Implications for nursing. Advances in Nursing Science, 5(4), 21-30.
Spiesschaert, Frans (2005). Ervaringsdeskundige in armoede en sociale uitsluiting. Een inleiding tot de methodiek [Experience expert in poverty and social exclusion. An introduction to the methodology]. Leuven/Amersfoort: Acco.
Suijs, Stijn (2012). Ervaring aan de grens. Hedendaagse armoedebestrijding in Vlaanderen [Experience at the border. Contemporary poverty reduction in Flanders]. Thesis, Katholieke Universiteit Leuven, Belgium, https://lirias.kuleuven.be/retrieve/194719 [Accessed: October 6, 2019].
Thomas, Sandra P. (2012). Examining nurse-to-nurse horizontal violence and nurse-to-student vertical violence through the lens of phenomenology. In Dave Holmes, Trudy Rudge & Amélie Perron (Eds.), (Re) Thinking violence in health care settings: A critical approach (pp.143-161). Burlington, VT: Ashgate.
van der Vaart, Gwenda; van Hoven, Bettina & Huigen, Paulus (2018). Creative and arts-based research methods in academic research. Lessons from a participatory research project in The Netherlands. Forum Qualitative Sozialforschung / Forum: Qualitative Social Research, 19(2), Art. 19, https://doi.org/10.17169/fqs-19.2.2961 [Accessed: October 6, 2019].
Van Nes, Fenna; Abma, Tineke; Jonsson, Hans & Deeg, Dorly (2010). Language differences in qualitative research. Is meaning lost in translation?. European Journal of Aging, 7(4), 313-316, https://doi.org/10.1007/s10433-010-0168-y [Accessed: October 6, 2019].
Van Regenmortel, Tine (2002). Empowerment en maatzorg [Empowerment and customized care]. Leuven: Acco.
Van Regenmortel Tine & Fret, Ludo (2000), Van moralisme tot empowerment als ethisch perspectief binnen het welzijnswerk en van armoedebestrijding [From moralism to empowerment as an ethical perspective within welfare work and from poverty reduction]. In Jan Vranken, Dirk Geldof & Gerard Van Menxel (Eds.), Armoede en sociale uitsluiting [Poverty and social exclusion] (pp.291-313). Leuven/Amersfroot: Acco.
Vitus, Kathrine; Thuesen, Frederiek & Tanggaard, Lene (2014). Konflikt i kvalitative studier – hvorfor og hvordan? [Conflict in qualitative research—why and how?]. In Lene Tanggaard, Frederiek Thuesen & Kathrine Vitus (Eds.), Konflik i kvalitative studier [Conflict in qualitative research] (pp.15-36). Kopenhagen: Hans Reitzels Forlag.
Wallerstein, Nina (1992). Powerlessness, empowerment, and health: Implications for health promotion programs. American Journal of Health Promotion, 6(3), 197-205.
Wang, Caroline & Burris, Mary Ann (1994). Empowerment through photo novella: Portraits of participation. Health Education Quarterly, 21(2), 171-186.
Wang, Caroline C.; Yi, Wu Kun; Tao, Zhan Wen & Carovano, Kathryn (1998). Photovoice as a participatory health promotion strategy. Health Promotion International, 13(1), 75-86, https://doi.org/10.1093/heapro/13.1.75 [Accessed: October 6, 2019].
Woodgate, Roberta L.; Zurba, Melanie & Tennent, Pauline (2017). A day in the life of a young person with anxiety: Arts-based boundary objects used to communicate the results of health research. Forum Qualitative Sozialforschung / Forum: Qualitative Social Research, 18(3), Art. 17, http://dx.doi.org/10.17169/fqs-18.3.2886 [Accessed: October 6, 2019].
Wright, Michael & Kongats, Krystyna (Eds.) (2018). Participatory health research voices from around the world. Berlin: Springer.
Guiney Yallop, John J.; Lopez de Vallejo, Irene & Wright, Peter R. (2008). Editorial: Overview of the performative social science special Issue. Forum Qualitative Sozialforschung / Forum: Qualitative Social Research, 9(2), Art. 64, http://dx.doi.org/10.17169/fqs-9.2.375 [Accessed: October 6, 2019].
Zimmerman, Marc A. (2000). Empowerment theory. In Julian Rappaport & Edward Seidman (Eds.), Handbook of community psychology (pp.43-63). Boston, MA: Springer.
Barbara GROOT is a researcher at Amsterdam UMC, VU University Medical Centre, Department of Medical Humanities, The Netherlands. She works on her thesis on participatory health research and ethics. Barbara coordinates the Centre of Client Experiences in Amsterdam and is involved in many participatory research projects in different sectors. She teaches participatory and qualitative research.
Contact:
Barbara Groot
Department Medical HumanitiesAmsterdam UMC, VUmc, Amsterdam Public Health InstituteDe Boelelaan 1089a, 1081 HV Amsterdam, the Netherlands
Tel.: 0031-6 15907823
E-mail: b.groot@amsterdamumc.nl
URL: http://www.CentrumvoorClientervaringen.com and http://www.SchoolforParticipation.com
Tineke ABMA is a professor for participation & diversity and senior researcher at the Amsterdam Amsterdam Public Health Institute. Tineke is a member of the ICPHR consortium and worked lately on two books with others about "Evaluation for a Caring Society" and "Participatory Research of Health and Well-being."
Contact:
Tineke Abma
Department Medical HumanitiesAmsterdam UMC, VUmc, Amsterdam Public Health InstituteDe Boelelaan 1089a, 1081 HV Amsterdam, the Netherlands
Tel.: 0031-20 4448266
E-mail: t.abma@amsterdamumc.nl
Groot, Barbara C. & Abma, Tineke A. (2020). Participatory Health Research With Mothers Living in Poverty in the Netherlands: Pathways and Challenges to Strengthen Empowerment [59 paragraphs]. Forum Qualitative Sozialforschung / Forum: Qualitative Social Research, 21(1), Art. 8, http://dx.doi.org/10.17169/fqs-21.1.3302.

Creative Commons Attribution 4.0 International License